I see many, many women for implant removal after years of being unhappy with their breast implants. Many of these ladies consulted a plastic surgeon for sagging of the breasts and instead of ending up with a breast lift, ended up with breast implants. Often the explanation for this is that the patient did not want the “scars of a breast lift”.
So here’s the deal on breast lift scars. Yes, they are more extensive than the scars from an augmentation but,………………………..in the vast majority of patients, the scars fade to near no-big-deal status in about a year. Check out the example shown. The top photo is before a lift, the middle photo about 6 months post op and the bottom photo is one year post op. See the scar? Well you hardly can see the scars in the bottom photo. This is not an exceptional case. This is usually how it goes. Now there are some rare individuals who scar badly because of their particular biology but they are the exception.
So………….if you are saggy, you should get a lift. If you are really small you should get an augmentation with either an implant or fat transfer. As with everything, the correct diagnosis should lead to the correct treatment.
Thanks for reading and follow me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
I participate in a few doctor only on line message boards and forums. A topic that has been front and center the past few months has been the #METOO movement and some of the challenges women in medicine face. I’d like to share a few of my own stories. Fortunately none of them include Harvey Weinstein.
I finished medical school in 1983. 1/3 of my graduating class were women. These days women comprise more than 50% of most medical school classes. I did my general surgery residence at the University of Utah, not exactly a bastion of progressive ideas. Surprisingly about 20% of the surgery residents were women. I felt very little discrimination but maybe I was just to busy and exhausted to notice? I did get a couple of evaluations that I thought were just hilarious and still do. They were both from the Latter Day Saints (Mormon) Hospital. One described me as “defensive, argumentative and with a chip on my shoulder”. The other described me as “a sharp little gal”. My boyfriend at the time just about split a gut laughing when he saw these. He was also a general surgery resident and never got such amusing reviews.
I had a few interesting experiences with male patients. When I was doing an Intensive Care Unit rotation as a wet behind the ears intern at the University Hospital, I helped with a middle aged Mormon Elder who was crashing badly from acute pancreatitis. (If you have never heard of this disease, count yourself lucky). I was cleaning his penis in preparation to place a catheter so we could monitor his urinary output. This man was very ill and a little delirious. He looked at me and said “Doc, I’ll give you 10 minutes to stop that”. It never crossed my mind to take offense at this. It added a bit of levity (ha, ha) to a very serious situation. I got to know this gentleman quite well during his ICU stay and he was a totally stand up guy. On the gastroenterology rotation during my third year, I was doing a colonoscopy on an elderly man and he twisted his torso and neck to look me right in the eye and asked “What is a pretty little thing like you doing here?” At the time, I thought that was actually a very good question! This fellow grew up in a time where women rarely worked outside the home and certainly did not become surgeons. Again, since I was the one with the scope, I felt no animosity towards him.
Dr. Henry Neal in 1990 with his girl residents, me, Sue Wermerling and Kimberley Goh. Can you tell that he secretly loves us?
My first year of my plastic surgery residency (after 6 years of general surgery) three of the four residents were women. This was a fluke of the computer based residency matching system. The chairman of plastic surgery, Dr. Henry Neale was a good old boy from the south. He kept a bull whip in his desk drawer. Really. He was a great surgeon and ran a powerful department. We operated our brains out and he had our back every day. Dr. Neale was very, very politically incorrect. He pondered if Sue, Kim and I would start cycling together and once stated he should put a Kotex machine in the resident’s office. Well, the three of us just dished it right back at him and we did end up cycling together.
There was one occasion where I really felt harassed. I was a 4th year general surgery resident on call at a private hospital in Ogden, Utah. Late one night there was knock on my call room door. I opened it to find an elderly staff surgeon with alcohol on his breath with a fifth of Southern Comfort (yuck!) in his hand. He wanted to know if I wanted to party. This scene was so ludicrous that I laugh out loud just thinking about it. Most residents given the choice of sleep vs. party would pick sleep no matter whom was holding the bottle. This man’s son was a medical student who had rotated on my service a few months previously. I told the party hound horn dog that he had three seconds to leave or I would tell his son. I think he was gone before I hit “two”. I never assisted him on a case again which was no loss on my part because he was a lousy surgeon. No, I did not file a complaint or make a fuss of this. Again, he grew up in a different time.
I’ve had a few really weird patient encounters in private practice related to my gender. Years ago when I was pregnant with my twin sons and could barely fit through a door, I had a mentally unstable older man with a skin cancer on his scalp the size of a poker chip. This, gentle readers, is what we surgeons call a GREAT CASE. The mentally unstable older man was quite the cad with many comments about my huge belly and the certain studhood of my husband. He also had many bizarre ideas about selenium deficinecy and sexual function. I was not sad to send him on his way once he had healed. A few years later I had an elderly woman come in with another neglected and ginormous skin cancer who shrieked when she saw me and declared that “women are stupid and I won’t have one for my doctor”. Oh well, that great case went to my partner who has a Y chromosome. She was nasty to him too.
As I write this blog, I can’t really think of any weird encounters in recent years. I think in the 26(!) years since I started practice that being a woman surgeon or woman astronaut or woman programmer or even race car driver has become sort of a no big deal which suits me just fine. Recently my 17 year-old daughter took a field trip with her computer science class to the Microsoft campus just outside of Seattle. She attends an all girl high school and they were given a tour by an all female coding team. The advice given to these bright young students by these bright young and not-so-young techies was to work hard, advocate for yourself and don’t take things too personally. I think that is good advice regardless of your gender or your workplace.
Thanks for reading and follow me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder, girl surgeon. And there will be an upcoming blog about delayed childbearing which is something I don’t recommend but sure worked for me.
I belong to a few physician only message boards and breast implant illness has been a hot topic in the past few months. It is interesting to see what other plastic surgeons think and especially what physicians in other specialties think about this controversial topic. These boards encourage free discussion without anyone being shut down, banished, blocked, or slammed on social media. This makes me grateful to be part of a group of professionals that value serious and candid discussion of complicated issues. Here I present a few thoughts I have curated from the past several months.
Dry eye and breast implants: Many, many ophthalmologists weighed in on this one. The consensus is that dry eye is very common in middle aged women. Women are 10 times more likely to develop dry eye. One doc said 80% of his female patients over 50 had dry eye. Conditions that contribute to dry eye include previous eyelid surgery (blepharoplasty), too much screen time, and some medications including SSRI antidepressants. Implants? No support for that theory from any of the ophthalmologists. My ophthalmologist, who recently did my cataract surgery, looked at me like I was nuts when I asked him about implants and dry eye. The eye docs also reminded us that silicone products are used extensively in ophthalmology: punctal plugs for dry eye, silicone stents for nasolacrimal duct reconstruction, silicone buckles used to treat retinal detachment, silicone oil used as a replacement for vitreous humor in the posterior chamber (eyeball), silicone intraocular lenses used after cataract extraction and finally silicone contact lenses. WOW. That’s a boat load of silicone.
When docs congregate is it wisdom of the crowd or groupthink?
Mold and biotoxins: General consensus from internal medicine and infectious disease is that patients ill with systemic fungal infections should be in the intensive care unit. None of the plastic surgeons, with one exception, had seen a case of mold growing in a saline implant. I added up the years of practice and it came to about 250 years. That is a lot of experience. One plastic surgeon who has written a book on BII seems to see mold and biotoxins wherever she looks. She puts her implant removal patients on extensive anti-fungal therapy post-operatively. She has extensive experience with mold and biotoxins but has not been published in any recognized peer reviewed medical journals. Her reason for not doing so has something to do with being targeted by Big Pharma. Hmmm.
Autoimmune issues: There were several rheumatologists weighing in on silicone triggered illness. Their opinions varied from no evidence whatsoever to there are some individuals who are genetically susceptible to autoimmune diseases (this is well known) and exposure to silicone may trigger the onset of disease in these individuals. It was noted that women are affected by autoimmune disease about 4 times more commonly than men. One infectious disease doctor thinks breast implants caused slceroderma (which is very, very serious connective tissue disorder and is usually fatal) in 6 of his patients. He recommended checking how wide an implant patient can open her mouth to diagnose early perioral and TMJ fibrosis and scleroderma. The rheumatologists thought that this doc was really out there. The plastic surgeon who has written a book on BII, who is not a rheumatologist, stated that rheumatoid arthritis is caused by an intracellular mycoplasma infection and she can cure rheumatoid arthritis and scleroderma with non-conventional therapy. None of the rheumatologists believed her. They all wondered why she had not published her results in a peer reviewed medical journal. Same answer. Big Pharma.
Breast Implant Associated Anaplastic Large Cell Lymphoma: It is rare. It is treatable if caught early. It is really creepy. It is associated with textured breast implants and/or tissue expanders. The plastic surgeon who wrote the BII book stated that BIA-ALCL was the most common cause of death in her implant patients prior to 2005. It was pointed out by several other doctors that BIA-ALCL was recognized as a disease around 2012.
Other stuff: Many of the internal medicine docs, ER docs, pain specialists, psychiatrists and OB-gyns weighed in on so called functional and somatic disorders including fibromyalgia, chronic fatigue syndrome, pelvic congestion, brain fog, anxiety, poor memory. depression, and malaise as primarily affecting women and pointed out that the vast majority of these women with these disorders do not have breast implants. This chatter of functional and somatic disorders made me think of the Freudian disorder of “hysteria” of yesteryear which was supposedly caused by the uterus wandering around looking for a baby. This sort of stuff gets my hackles up a bit, being a woman and all. One doctor wondered if there were any male to female transgender individuals with breast implant illness. Now that is a great question.
Future research: Everyone pretty much agreed that a large, multi-center, long term (10+ years) may help answer many questions about breast implants. Several plastic surgeons, myself included, pointed out that the dismal long term follow-up in previous studies was in part due to patient non-compliance with follow-up. I know this will make a lot of people angry but it is really true. Back when gel implants were only available through studies like the one I participated in, once patients had their coveted gel implant, they were gone, gone, gone. My follow-up for the McGahn study was about 80% which is really high because my staff and I pestered the participants mercilessly to come in for their appointments. Once doc suggested maybe a prison study using inmates with really long sentences. Maybe this could be Orange in the New Black meets Extreme Makeover?
Breast implants in general: Whoa, were there some strong opinions about this. Many, many non-plastic surgeons think any woman who gets implants is by definition is a mentally impaired bimbo. One doc divulged that his wife was going to get implants to treat her postpartum atrophy and boy did he get an earful! Many of the male doctors assumed that she was preparing to leave him once he had paid for her surgery! Such cynicism. But there was one family practitioner who has had the same set of implants for over 30 years (!) who said they absolutely changed her life. She went from a wallflower to a confident young woman. She even credits her implants for giving her the confidence to apply to medical school!
Plastic surgery and plastic surgeons in general: Some of the docs think that any sort of appearance altering surgery (except for obvious reconstructive procedures) was morally and intellectually bankrupt. This was an opinion shared by many anesthesiologists! Weird, huh? I wonder if my anesthesia group thinks they are slumming to work in my OR? I guess I should ask. Many of the male docs stated they didn’t need plastic surgery because their female partners found them totally smokin’ hot just the way they are. Hmmmm. Some of the docs think we plastic surgeons are a bunch of money grubbing fools. Oh well. I chalk that one up to jealousy. ; )
So there you have my carefully collected and curated review of some wild times on the doctor only message boards. You too can join a doctors only message board but first you have to finish medical school.
Thanks for reading and check out my Instagrams @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
Is he certified by the American Board of Plastic Surgery? It would be in a patient’s best interest to check!
Real Seattle Real Plastic Real Surgeon blogs about the difference between a real plastic surgeon and a wannabe.
I participate in a physician only message and discussion board called Sermo. Lately there have been many discussions about the dangers of plastic surgery performed by doctors who are either poorly trained or, in some cases, not trained at all in surgery. These doctors may be trained in pediatrics, ophthalmology, family practice, radiology, OB-gyn or even occupational medicine. The things these doctors do have in common is that they have not completed formal and rigorous training in plastic surgery and they do not have hospital privileges for plastic surgery. They do their procedures under local anesthetic (this way they do not have to have their facility inspected or accredited) and they don’t know what they don’t know. It’s that “don’t know what they don’t know” that really scares me. It should also scare you.
Before signing up for surgery, check to make sure your doctor has hospital operating privileges and is certified by the American Board of Plastic Surgery – the only plastic surgery board recognized by the American Board of Medical Specialties. Accept no substitute!
Thanks for reading, Dr. Lisa Lynn Sowder, certified by the American Board of Plastic Surgery. Follwow me on Instagram @sowdermd and @breastimplantsanity.
K (Ryan Gosling) and the very evil Luv (Sylvia Hoeks) stroll among the newly finished small breasted replicants.
My husband and I went to Blade Runner 2049 this past weekend at Seattle’s wonderful Majestic Bay Theater. I am a big fan of the original Blade Runner thus the bar was very, very high for 2049. IMHO, Blade Runner 2049 was too frenetic, too convoluted and the only characters I really cared much about was Rick Deckard (the still handsome and wiley Harrison Ford) and his big ass shaggy mongrel doggie. I shed a tear when the doggie is shown peering out of a shattered building, wagging his tail just a bit, wondering where his human went. I’m tearing up now just remembering that scene.
One thing I found interesting throughout the movie was the relatively smallish breasts of all of the female characters. Hardly any cleavage at all – a real change for Hollywood. K’s (played by a deliciously disheveled Ryan Gosling) made-to-order AI concubine Joi (Anade Armas) and her human side kick, Mariette (Mackenzie Davis) with whom she mind and body melds, were both small chested. The LAPD’s Madame played by the ever wonderful Robin Wright was lean and mean and small chested. The still-under-construction and just “born” female replicants would all measure into an A or B cup bra. Even the gigantic virtual reality pleasure girl with the pastel hair was small breasted. The only bouncing breasts seen in the movie was in the cocktail lounge hologram dancing girls of the distant past. They contrasted nicely with Deckard and K beating the bejesus out of each other.
So maybe this return to a natural sized breast will be the next not-so-big thing for the ever scrutinized female figure?
Thanks for reading and if you haven’t seen the original Bland Runner, you are missing out on a great movie. Follow me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
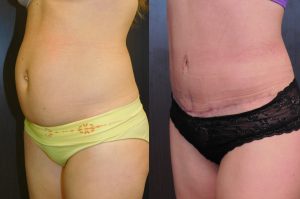
This patient had more muscle laxity that skin laxity. Here she is at 3 months with a very flat tummy. Her scar will fade with time.
I just love doing tummy tucks because this procedure allows me to tighten skin, fix muscle position, remove fat and improve a belly button in one operation. Usually this can be done with an incision that is admittedly quite long but is where the sun doesn’t usually shine. But sometimes, maybe 10% of cases, it is necessary to leave a scar in the lower mid-line. Sometimes a patient really needs a full tummy tuck to correct muscle separation but doesn’t have quite enough skin laxity of remove all of the skin between the pubis and the belly button and in those cases a “t-incision” is necessary. In most cases, I have a pretty good idea before surgery if I am going to need a t-incision but once in a while I cannot quite get that skin to stretch enough and have to leave a t-incision without prior warning to the patient. This occurred recently and I had a husband hopping mad at me for the extra scar. The alternative would have been to make the abdominal skin closure so tight that the patient would never be able to stand up straight again or position the really long horizontal scar quite high which would probably look worse than a nicely healed t-incision.
These intraoperative decisions are very, very difficult and sometimes, quite frankly, agonizing. I am hoping that this particular patient heals well and her vertical scar becomes a non-issue as is usually the case. And sometimes I just wish patients and their families could spend a day in my operating room clogs. It’s not so easy!
Thanks for reading and letting me get that one off my chest! Dr. Lisa Lynn Sowder
Follow me on Instagram @somdermd and @breastimplantsanity
This cartoon is by the late, great B. Kliban. His book, “Never Eat Anything Bigger Than Your Head” is a treasure. Get your hands on one if you can. You’ll laugh until you cry.
Portion control is very important for maintaining a healthy weight and it becomes more and more difficult as restaurants, especially fast food restaurants, keep increasing the size of the offerings. There is a Mexican place in Seattle that has a poster of one of its burritos next to a new born baby. They are the same size. So sick in so many ways, huh?
I would like to introduce portion control for breast implants. There is a condition that we plastic surgeon’s call breast greed. Those with breast greed want to go a little larger and then a little larger and then a little larger. This results in the eager to please plastic surgeon putting a too big implant into a too little woman. Supersized implants have an increased chance of having implant problems. Big implants cause thinning of the breast tissue and skin and over-stretching of the pectoralis muscle if they are submuscular. They are more likely to result in the dreaded unaboob or extend into the underarm area. And, in my humble opinion, they look really, really bizarre.
Fortunately I do not get many patients looking for that super top heavy look. Implant patients self select surgeons who feature these jumbo implants on their website or social media accounts. You won’t fine many of those attached to my name.
Thanks for reading and if you want to supersize your chest, don’t come to me! Dr. Lisa Lynn Sowder
Follow me on Instagram @sowdermd and @breastimplantsanity.
This lady initially came in for breast augmentation. She wanted to look a little fuller but was a worried about the impact of larger breasts on her competitive tennis game. After chatting with her and examining her, I came up with the plan of a lift and a nipple reduction. These procedures would give the illusion of fuller breasts without actually increasing the volume.
A small and saggy breast with a long stretched-out nipple looks – I’m gonna say it – a little pathetic. Once the breast skin is tightened up and the nipple shortened, the breast looks almost the way it did before babies, breast feeding, gravity, general aging, etc. And a procedure like this is maintenance free. It should last a lifetime. But remember to wear a bra most of the time when upright. Gravity never sleeps.
Thanks for reading! Dr. Lisa Lynn Sowder
Follow me on Instagram @sowdermd and @breastimplantsanity.
Can’t tell which side is anatomic and which side is round? Neither can I!
I think the anatomic implants vs. round implants smack down may finally be over. As those who read my blog know, I am not a huge fan of anatomic implants although I have tried really, really hard to learn to love them over many, many years. Anatomic implants are presented as the best thing since microwave nachos and those of us who keep going back to round implants are sometimes dismissed as Luddites. Anatomic implants are pushed by industry paid “experts” who make the rounds at meetings and extol the wonder of these more-expensive-and-more-complicated-than-round implants. And patients ask for these anatomic implants being lead to believe that they will look more natural.
A few years ago, evidence started trickling in that anatomic implants actually did not have advantages over round implants in standard breast augmentation in anatomically normal women. There were studies where before and after photos were shown to expert plastic surgeons and they could not tell which patients had which implants. I was present at one of these sessions where a panel of experts did no better than a coin toss. But the study that nobody thought could be done – put an anatomic in one side and a round in the other side on the same patient – has been done! No patient would sign up for having two differently shaped implants used for her augmentation and no institutional review board would approve such a study. But some very clever surgeons did this study in 75 volunteers. Their average age was 39 and their average BMI was 20 (this, by the way, is quite thin). The surgeons took the patients to the OR and put a round implant in one side and a comparably sized anatomic implant in the other side and then took standardized photographs. They then removed the anatomic implant and replaced it with a round implant to match the other side. The standardized photographs were shown to a panel of experts. Even the panel of experts could not tell the round vs. the anatomic when presented with these side by side breast implants!
I really take my hat off to the Drs. Hidalgo and Weinstein for doing this study. It is this sort of research that helps us make decisions based on reality rather than the latest hype from an industry hired gun.
Intraoperative Comparison of Anatomical versus Round Implants in Breast Augmentation: A Randomized Controlled Trial. Hidalgo, David A. M.D.: Weinstein, Andrew L. M.S., Plastic & Reconstructive Surgery: March 2017, Pages 587-596.
Seattle Plastic Surgeon (and mother of three) Dr. Lisa Lynn Sowder you about lawn mower safety.
It was such a wonderful thing to get some yard work out of my offspring once that they were old enough to mow, rake, sweep, weed, water, trim, edge, poop scoop, etc. As much as I loved the smell of newly mown grass and the thought of them working (instead of me), I worried. I worried about the lawn mower thus the little nag session each and every time one of my boys was nagged into mowing the lawn.
Here is my list of lawn mower safety tips.
Only children over 13 should mow a lawn.
One person only should be on the lawn being mowed. That would be the person behind or on the mower.
NO PETS unless it’s a rabbit you really wish you had never adopted.
Always wear socks and heavy shoes and gloves.
Always wear eye protection.
Ear plugs okay but not earbuds for listening to Bad Bunny’s greatest hits. They need to hear you yell, “Watch out for the dog!”
No mowing until the offspring has cooled down from his/her rage at having to actually perform agreed upon chores for agreed upon bennies. Rage and lawn mowers should never coexist.
If the mower malfunctions, turn it off and don’t even think about flipping it over unless a knowledgeable and responsible adult is present.
Leave sharpening to the experts. Oh, unless you work in a lawn mover sharpening shop, you are not an expert.
No using the lawn mover for anything other than mowing the lawn. This calls for a cautionary tale: Two patients in the same day present with nearly identical lawn mower injuries sustained while attempting to trim a hedge with a lawn mower. Patient #2 happen to see patient #1 (prior to his mishap) trimming his hedge with the lawn mower while Patient #2 was driving to get gas for his lawn mower and thought “Hey, what a great idea.” Not. This cautionary tale was told to me by an esteemed colleague practicing in Spokane, Washington many years ago. Being Spokane born and raised, I have every reason to believe it is 100% true.
Stay tuned. One of these blogs I will tell you about my dad’s snowblower injury. His bloody glove is still nailed to the wall of his shop some 30 years later.
 Many of these ladies consulted a plastic surgeon for sagging of the breasts and instead of ending up with a breast lift, ended up with breast implants. Often the explanation for this is that the patient did not want the “scars of a breast lift”.
Many of these ladies consulted a plastic surgeon for sagging of the breasts and instead of ending up with a breast lift, ended up with breast implants. Often the explanation for this is that the patient did not want the “scars of a breast lift”.


 After chatting with her and examining her, I came up with the plan of a lift and a nipple reduction. These procedures would give the illusion of fuller breasts without actually increasing the volume.
After chatting with her and examining her, I came up with the plan of a lift and a nipple reduction. These procedures would give the illusion of fuller breasts without actually increasing the volume.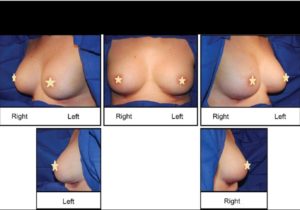


 @lisalynnsowder
@lisalynnsowder
