It’s that time of year again. Roll up your sleeve and get your flu shot already. Why should a “surgical sub-specialist” like me care about whether or not you’ve had your flu shot? First of all, I’m a physician and it is my duty promote good health. Second of all, I don’t want any of my patients coming down with the flu. If a patient falls sick before surgery, we have to cancel and then reschedule the case which is hard on us meaning surgeons, anesthesiologists, surgical techs and nurses and it is also really hard on the patient because he/she has to carve more time out of a busy schedule and many times arrange for child care, not only for surgery but for recovery.
If a patient comes down with the flu in the early postoperative period, he/she may end up wishing they had never been born. That would make for a less than excellent plastic surgery experience and could also be down right dangerous.
And we tend to think of the flu as just an inconvenience with a little misery added but really, the flu can be very, very serious. I am old enough to remember the Hong Kong Flu of 1968. I was sicker than a dog and missed a week of school but was not one of unlucky million or so who died. And then there was a Spanish Flu of 1918 that killed 50 (!) million mostly healthy, young people. Sorry to be such a fear monger but I really want you to get a flu shot.
Seattle Plastic Surgeon blogs about fillers she does not like and does not use.
I’ve written many blogs on the miracles of fillers for facial aging. I think they are the best thing for facial maintenance since sunscreen.
Facial silicone gone bad. Really, really bad.
The fillers I really like and use a lot are Voluma, Juvederm, Restylane, and Perlane which are all hyaluronic acid (HA) fillers. The thing I love about HA fillers is their ease of use, safety, and their reversibility when a rare patient (1 every five years or so) does not like the result. The HA fillers can be reversed by injecting an enzyme which dissolves the filler within 24 hours.
I also use fat as a facial filler in some cases. The thing I like about fat is that there is usually an abundant supply and it is often very, very long lasting and sometimes permanent.
There are other fillers out there. Here’s my list of fillers that I just don’t like or use. Full disclosure here: this is based solely on my (sometimes very limited) experience, hearsay, prejudice and my risk adverse nature. Some of my colleagues use these regularly and successfully but these fillers just give me the creeps.
Collagen: It is sooooo yesteryear. Even when it was the only legit filler out there, I didn’t like it. Patients needed a skin test 30 days prior to using Collagen. The results were fleeting and even a detail freak like me had trouble getting a nice smooth result. Oh, it also had to be refrigerated and shelf life was very limited. Oh, one more thing, it comes from cows.
Radiesse: This is used quite a bit in the Seattle area but it gives me the creeps. It’s made of teeny, tiny spheres of calcium hydroxylapatite and provides a scaffold for connective tissue growth. It is quite thick and can fill in deep creases nicely but can also result in nodule formation. Radiesse lasts 1 -2 years which is great (unless you are one of the unlucky ones who develops nodules). I used it a few times years ago in a a few employees who volunteered (really, they did) to be my training subjects. All three of them bruised really, really badly and I felt like a worm until their bruising resolved. I don’t have a cajones to try it again.
ArteFill: Yikes. This is a scary one. This is a permanent filler which is made up of teeny, tiny spheres of polymethylmethacrylate. They elicit a “foreign body response” which walls off the little spheres with collagen. It also requires a skin test 30 days before injection because the sphere are carried in liquid collagen. My training subjects this time were two pals of mine. Both had negative skin tests. My first patient did fine and is still my pal. The second patient, who was from out of state, had to delay her injection because a family illness prevented her from traveling. Four months later, she had a rip-roaring inflammatory reaction to the little spot on her forearm where I had injected the test dose. It was by the grace of a good and loving God I had not injected her face. She is still one of my very best pals. I have also seen many case reports and a couple of patients with poor results from ArteFill. The only way to get rid of it is to surgically remove it.
Sculptra: Sculptra stimulates dermal fibrosis and thickens the skin. This is filler was first introduced about 10 years ago for use in patients with HIV. The medications that many HIV patients rely upon to stay healthy have the side effect of facial wasting. This filler is made of poly-L-lactic acid, the same chemical that a common suture, Vicryl, is made of. I use Vicryl a lot. It is easy to sew with. It provides strength and support for a couple of months while an incision heals and then the body absorbs sit. But once in awhile, a patient has an inflammatory reaction to the suture. I have had maybe a dozen patients over 20 + years of practice who have “spit” every single stitch. There are many case reports of disfiguring inflammatory reactions to Sculptra and all I have to do is think of one of my Vicryl “allergic” patients and I break out into a cold sweat. Am I a wimp or what?
Silicone: This is the Queen Mother of Bad Fillers (in my humble opinion). It has been used for decades and is responsible for the permanent disfiguration of many, many patients. I will never forget a lecture I attended when I was a surgery resident on the treatment of a bizarre condition called Romberg’s disease. This disease causes profound atrophy of facial fat. Way back when, these patients were injected with medical grade silicone and initially it was beneficial. But fast forward 10, 20 even 30 years and many of these patients went on to develop severe inflammatory reactions that were more disfiguring than the original disease. I know of a plastic surgeon in Hawaii who used this stuff on his wife’s lips. Yikes.
So there is my personal rogue gallery of “no thanks” fillers. All of these (I think) are still in the good graces of the F.D.A. but you won’t find them on my shelf.
Hey, thanks for reading. That was a slog, wasn’t it? Dr. Lisa Lynn Sowder
Seattle Plastic Surgeon (and mother of three) Dr. Lisa Lynn Sowder you about lawn mower safety.
It was such a wonderful thing to get some yard work out of my offspring once that they were old enough to mow, rake, sweep, weed, water, trim, edge, poop scoop, etc. As much as I loved the smell of newly mown grass and the thought of them working (instead of me), I worried. I worried about the lawn mower thus the little nag session each and every time one of my boys was nagged into mowing the lawn.
Here is my list of lawn mower safety tips.
Only children over 13 should mow a lawn.
One person only should be on the lawn being mowed. That would be the person behind or on the mower.
NO PETS unless it’s a rabbit you really wish you had never adopted.
Always wear socks and heavy shoes and gloves.
Always wear eye protection.
Ear plugs okay but not earbuds for listening to Bad Bunny’s greatest hits. They need to hear you yell, “Watch out for the dog!”
No mowing until the offspring has cooled down from his/her rage at having to actually perform agreed upon chores for agreed upon bennies. Rage and lawn mowers should never coexist.
If the mower malfunctions, turn it off and don’t even think about flipping it over unless a knowledgeable and responsible adult is present.
Leave sharpening to the experts. Oh, unless you work in a lawn mover sharpening shop, you are not an expert.
No using the lawn mover for anything other than mowing the lawn. This calls for a cautionary tale: Two patients in the same day present with nearly identical lawn mower injuries sustained while attempting to trim a hedge with a lawn mower. Patient #2 happen to see patient #1 (prior to his mishap) trimming his hedge with the lawn mower while Patient #2 was driving to get gas for his lawn mower and thought “Hey, what a great idea.” Not. This cautionary tale was told to me by an esteemed colleague practicing in Spokane, Washington many years ago. Being Spokane born and raised, I have every reason to believe it is 100% true.
Stay tuned. One of these blogs I will tell you about my dad’s snowblower injury. His bloody glove is still nailed to the wall of his shop some 30 years later.
MRI is the best test for detecting implant rupture (other than surgery) with a very high accuracy rate, much higher and mammogram, ultra sound or physical exam. I think it is prudent for patients with gel implants, say 10 years old or older to get an MRI to make sure there is not a silent rupture. If a patient has saline implants, there is no possibility of a silent rupture so an MRI would be worthless unless there is another reason for MRI (cancer detection for example). I often have patients who are coming in to have their old gel implants removed regardless if they are intact or ruptured and in those cases I don’t really think an MRI is absolutely necessary. Yes, it is nice for the surgeon to know ahead of time if there is a rupture but honestly, I approach every implant removal as if the implant is ruptured. I try to do an en block resection and have everything ready in the event the implant is ruptured and there is silicone spillage. We have special suction set up for ruptured implants and also some old fashioned surgical lap pads ready for clean up. And even with a rupture, it’s usually not as messy and one might think it would be. Even the messiest cases almost always allow the surgeon to scoop out the gel and then get all of the capsule.
“Just relax. It doesn’t hurt one bit but it is a little noisy.”
In Seattle at Swedish Medical Center, as of 2017, an out-of-pocket MRI to rule out breast implant rupture is about $1300 – $2200. If you pay up front, you get the lower price. The actual procedure requires the patient to lie prone (on the stomach) with the breasts hanging though these little openings in the MRI bed. It’s important to lie really, really still for a good image. MRI does not involve any irradiation so don’t worry about that but it can be kinda noisy with pings and dings. When I had my knee scanned, they gave me earplugs. And after an MRI, please make sure you get the radiologist report. It is more useful than the actual MRI itself. Plastic surgeons are not experts at reading MRI’s although we can usually see an obvious rupture. More subtle things may not be obvious to us.
Thanks for reading and if you are concerned about your oldish gel implants and an MRI will either ease your mind or prod you into action, you should get one! If are ready to bid goodbye to your oldish implants regardless of their status, come on in. I’m here to help!
Thanks for reading! Dr. Lisa Lynn Sowder. Follow me on Instagram @sowdermd and @breastimplantsanity.
Seattle Plastic Surgeon Discusses Mommy Makeover on Mother’s Day
Ah, the joys of motherhood! I can wax eloquently about fat little feet, apple cheeks, wet baby kisses and so on but one of the joys I did not expect was a boost in my Plastic Surgery practice, especially my “mommy makeover” patients. Since becoming a mother myself, I speak “mommy” really well. I know first hand the glorious details of feeding, bathing, changing, and schlepping the baby. I can recite the stages of the toddler, the preschooler, the gradeschooler, the tween, the teenager and currently I am becoming an expert on the joys of being the mother of young adults.
Being familiar with all that being a mother requires makes me much better at counseling patients about the process and timing of a “mommy makeover”.
“Mommy makeovers” usually combine breast surgery (augmentation and/or lift or reduction) with body surgery (usually abdominoplasty and/or liposuction). Most women are healthy enough to have a combination of procedures during one operative session. It is, however, the first couple of post operative weeks that are the most challenging for the patient.
Mommy is used to taking care of everyone but herself. After surgery the Mommy needs to take of only herself. She needs to be “Queen for a Week or Two” and resist the urge to cook, clean, change, wipe, mop, vacuum, load, unload, fold, etc. And if her youngest weighs over 20 pounds, she may not pick him/her up for at least two weeks if breast surgery was done and for at least six weeks if an abdominoplasty was done. The little one can crawl into Mommy’s lap for a cuddle but NO HEAVY LIFTING for Mommy. This also applies to the dog.
It’s very important to for patients to discuss these issues with their families. I’ve had a few ladies who have underestimated their recovery time, have done too much too soon and have turned what should be a relatively comfortable and relaxing recovery into a very sore and frustrating one.
So, calling all mothers interested in a “mommy makeover”: Plan ahead and get your husband and your children and your friends on board. Make a sign for your bedroom door. “DO NOT DISTURB – MOMMY RECOVERING”.
The Placebo Effect and its evil twin, the Nocebo Effect.
I’ve been doing some interesting reading lately on the mind/body connection in preparation for a presentation I am giving at the annual meeting of the Northwest Society of Plastic Surgeons this month. I have been reading up on the “Nocebo Effect” which is the evil twin of the much studied and celebrated “Placebo Effect.” Any one who has kissed a child’s owie is well acquainted with the placebo effect.
The nocebo effect is a more recently studied phenomenon. One nocebo effect study involved giving a fake lactose solution to a group of participants which included lactose tolerant and lactose intolerant individuals. 44% of the lactose intolerant and 26% of the lactose tolerant reported gastrointestinal distress after ingesting the sham lactose. The study participants were told that the solution was know to cause gastrointestinal symptoms. The nocebo effect can be disruptive when it comes to new drug trials. In some cases almost 10% of the participants in the placebo arms of clinical trials have to drop the study because of adverse effects. I have come to view the nocebo effect as the Power of Negative Thinking. We humans are very susceptible to suggestion.
I had a patient recently who came in for removal of her surgical drains after a breast reduction. She was just a nervous wreck and was clearly bracing herself for the most painful thing ever. I asked her about her anxiety and she told me she had seen a YouTube video of a young man who had had a gynecomastia procedure getting his drains removed. He apparently was howling like an injured wolf. He must have either had a very low pain threshold or maybe he was a drama student? Anyway, while chatting with my patient, I slipped out her first drain in about 3 seconds. Then I slipped out the other one. She was pleasantly surprised at how quick and easy it was. Yes, it stung a little but no need for howling. The howling wolf video she saw was the nocebo effect at work. The nocebo effect is one reason I implore my patient to avoid surgery horror stories before and after their procedures. For every horror story out there are likely 10,000 undocumented stories of uneventful surgery and recovery. But uneventful isn’t nearly as interesting as a howling wolf.
Thanks for reading and beware the nocebo effect. Dr. Lisa Lynn Sowder.
Seattle Plastic Surgeon knows how to make the Grinch look a little less grinchy.
It’s those glabellar frown lines and nasolabial folds that make this Grinch look soooo grinchy.
Take a look at the Grinch. What is it that makes him look so old and cranky? It’s his glabellar from lines between his eyes that make him look like he’s having a pretty bad day and it’s his nasolabial folds (those creases that go from the sides of the nose to the corners of the mouth) that make him look a billion years old. All he needs to do to work himself up into a really bad mood is to look in the mirror every morning. No wonder he has such a bad attitude.
If the Grinch were to come into my office, here is what I would recommend:
His forehead creases would be softened and smoothed out with Botox. He looks like he needs a pretty large dose, maybe 60 units. The injection would sting but would be quick and he would see a remarkable improvement within 3 days or so. Also, he would feel so much more relaxed. If he wanted to scowl at his poor little dog, he would be unable to! Smile, yes but scowl, no. This amount of Botox would set him back $900 and would last at least 3 months. If he kept coming back for treatment, his dose would likely drop considerably.
His nasolabial folds could be filled in with one of the hyaluronic facial fillers that I inject almost every day of the week. They are terrific for treating the area around the mouth that is such a problem in some people and is hard to treat with other methods. Even a full face lift doesn’t help this area very much. I would use 2 or 3 syringes to get as full of correction as possible. It’s been my experience that patients who opt for just partial correction (to keep the cost down) are not nearly as satisfied as those who just go for it. Three syringes of a filler such as Juvederm would set him back about $1600. Juvederm lasts at least six months and I have many patients who have had nice lasting improvement for up to two years.
Do what about the redemption of his rotten soul? I’ll leave that up to the transcendent love and forgiveness of Whoville. But he’s got to save his face for me.
It is common to combine surgical procedures and often makes a lot of sense to do so. Combining procedures saves a trip to the operating room, saves some money and consolidates recovery time. Procedures often done in combination include breast lift with a tummy tuck and face lift with blepharoplasty.
There are some procedures, however, that I will not combine. Here is an example: Posterior hip liposuction and facial surgery. Why? Liposuction involves some heavy physical labor. I work up a sweat with most major liposuction cases. That heavy large muscle effort leaves me with a fine tremor for about an hour or so and I don’t want to do fine facial surgery with a fine tremor. So can’t I do the facial surgery first? No that won’t work either. The posterior hip liposuction requires the patient to be face down on the OR table. Positioning a patient who has just had facial surgery face down is NOT a good idea. Another example: Brachioplasty (upper arm lift) and tummy tuck is not a good combination. A tummy tuck really leaves the patient without core strength for several weeks so the patient is very reliant on the arms to move around in bed or get up from lying or sitting down. Arms that are fresh from a brachioplasty are very sore and should not engage in heavy work.
So, when patients are looking at more than one procedure, sometimes it makes sense to combine them but sometimes it doesn’t. Oh, and one other factor is surgeon fatigue. Yes, even badass surgeons like me get tired. More about that in another blog post.
Every week I get some questions sent to me by the website RealSelf. I am always amazed by the many questions submitted by patients sometimes within a day or two of surgery. I cannot fathom why a patient would turn to an online community of doctors rather than their own surgeon to answer their questions and address their concerns.
OMG. Is that going to happen to me?
And then there are patients who scrub the web for scenarios that are either much better or much worse than their own. I just don’t get it.
I advise my patients to concentrate on their situation, their surgery, their recovery. Going online and finding someone who is healing quicker than you or slower than you or just differently that you is not helpful and let me tell you, it makes your surgeon a little cranky.
So……………..take your meds as prescribed. Get some rest. Drink lots of water. Go out for a little walk. Make yourself a sandwich. Make your caregiver a sandwich. Clean our your junk drawer. Questions? Concerns? Run them by your surgeon. Just don’t go online.
Resusianne saved once again by Seattle Plastic Surgeon.
Last Saturday I had my biyearly Advanced Cardiac Life Support review and examination. After an excellent review of heart rhythms, various resuscitation drugs, much studying and fretting and sweating bullets while taking the written exam, I was taken into a small room by a seasoned and tough-as-nails intensive care unit nurse. There, on the table, lay Resusianne. After many years of saving her life, I just call her Anne for short. I don’t really care for her much but only because she makes me so nervous. You see, she is always trying to die on me.
Resusianne lives yet again.
My nurse examiner starts with the scenario that I’m in Nordstrom’s and come across a woman who is laying, unmoving on the floor. My first thought is sticker shock at the price of this bikini but I keep that to myself. I automatically go though the drill that has been beat into me over three decades.
“Anne! Anne! Are you okay?” Of course she’s not okay. Resusianne is never okay but it seems polite to ask. “I need help! Someone call 911 and someone bring an AED.” And then I start CPR. Now the fun starts when the AED arrives. I have to fumble for the on switch, rip open Anne’s shirt (fun!) and put on the paddles and then start CPR again until the AED tells me to stop. And then it seems like an hour before the AED decides to shock Anne. As soon as the shock is completed, I start in on CPR again until the nurse has mercy on me and tells me I can stop. Good CPR is really, really physical, especially for a petite little gal like me. By this time, I am a nervous wreck. I take Anne’s problems way too personally.
Normal Sinus Rhythm is a beautiful thing.
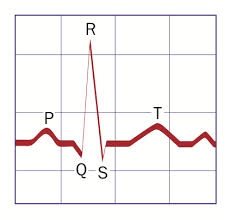
Next, my examiner gives me this scenario: I’m in the operating room with a patient and her EKG shows a heart rate that suddenly goes from 68 to 135 and her blood pressure starts to drop. This is the arrhythmia part of the test. You know that nice normal EKG pattern we always see with a spike between two humps? That is called normal sinus rhythm and that is what we love to see on an EKG but Anne is such a drama queen. She’s never in that rhythm for long. There are a dozen or so aberrant rhythms that range from kind of ugly to downright terrifying. Her current rhythm is somewhere in the middle and responds to a nice dose of Adenosine. She converts to normal sinus rhythm. Woo Hoo! But there she goes again. Fie on her. I give her a second and larger dose of Adenosine which really works this time. After Anne is conscious, I tell her that I will never, ever operate on her again and that she needs to find another plastic surgeon with larger cajones than mine.
And then my examiner raises the bar. This time Anne has just walked into my office to get her tummy tuck stitches out and she goes to ground right in the middle of my really nice waiting room! How rude. I go through all the steps of CPR and get EKG monitoring set up which shows normal sinus rhythm but Anne has no, nada, zero, zilch pulse. So now while I’m doing CPR and getting an IV started and pushing epinephrine I have to figure out why it is that Anne’s heart has electrical activity but is not pumping blood. There are about 12 reasons this can happen and I start with the most common in this scenario which is a pulmonary embolus (a blood clot to the lung). Now, after some IV fluid and epinephrine, Anne has a little bit of a blood pressure and I am ready to inset a breathing tube and get her over to Swedish Hospital for a diagnostic CAT scan and treatment and I’m about to have a cardiac arrest myself with my nurse examiner tells me that my exam is over and I passed! WOO HOO! I’m good for two more years and now I get to go change my scrubs which are soaked with sweat. I really, really hope I never have to use these skills. But I’m glad to keep up to date …..just in case. I say goodbye to the examiner but not to Anne. I may have a different examiner in two years but I know Anne will be back. She always is.
Thanks for reading and if you don’t know CPR, get thee to a class. The life you save my be of someone you love! Dr. Lisa Lynn Sowder










 @lisalynnsowder
@lisalynnsowder
