Seattle Plastic Surgeon knows how to make the Grinch look a little less grinchy.
It’s those glabellar frown lines and nasolabial folds that make this Grinch look soooo grinchy.
Take a look at the Grinch. What is it that makes him look so old and cranky? It’s his glabellar from lines between his eyes that make him look like he’s having a pretty bad day and it’s his nasolabial folds (those creases that go from the sides of the nose to the corners of the mouth) that make him look a billion years old. All he needs to do to work himself up into a really bad mood is to look in the mirror every morning. No wonder he has such a bad attitude.
If the Grinch were to come into my office, here is what I would recommend:
His forehead creases would be softened and smoothed out with Botox. He looks like he needs a pretty large dose, maybe 60 units. The injection would sting but would be quick and he would see a remarkable improvement within 3 days or so. Also, he would feel so much more relaxed. If he wanted to scowl at his poor little dog, he would be unable to! Smile, yes but scowl, no. This amount of Botox would set him back $900 and would last at least 3 months. If he kept coming back for treatment, his dose would likely drop considerably.
His nasolabial folds could be filled in with one of the hyaluronic facial fillers that I inject almost every day of the week. They are terrific for treating the area around the mouth that is such a problem in some people and is hard to treat with other methods. Even a full face lift doesn’t help this area very much. I would use 2 or 3 syringes to get as full of correction as possible. It’s been my experience that patients who opt for just partial correction (to keep the cost down) are not nearly as satisfied as those who just go for it. Three syringes of a filler such as Juvederm would set him back about $1600. Juvederm lasts at least six months and I have many patients who have had nice lasting improvement for up to two years.
Do what about the redemption of his rotten soul? I’ll leave that up to the transcendent love and forgiveness of Whoville. But he’s got to save his face for me.
It is common to combine surgical procedures and often makes a lot of sense to do so. Combining procedures saves a trip to the operating room, saves some money and consolidates recovery time. Procedures often done in combination include breast lift with a tummy tuck and face lift with blepharoplasty.
There are some procedures, however, that I will not combine. Here is an example: Posterior hip liposuction and facial surgery. Why? Liposuction involves some heavy physical labor. I work up a sweat with most major liposuction cases. That heavy large muscle effort leaves me with a fine tremor for about an hour or so and I don’t want to do fine facial surgery with a fine tremor. So can’t I do the facial surgery first? No that won’t work either. The posterior hip liposuction requires the patient to be face down on the OR table. Positioning a patient who has just had facial surgery face down is NOT a good idea. Another example: Brachioplasty (upper arm lift) and tummy tuck is not a good combination. A tummy tuck really leaves the patient without core strength for several weeks so the patient is very reliant on the arms to move around in bed or get up from lying or sitting down. Arms that are fresh from a brachioplasty are very sore and should not engage in heavy work.
So, when patients are looking at more than one procedure, sometimes it makes sense to combine them but sometimes it doesn’t. Oh, and one other factor is surgeon fatigue. Yes, even badass surgeons like me get tired. More about that in another blog post.
Resusianne saved once again by Seattle Plastic Surgeon.
Last Saturday I had my biyearly Advanced Cardiac Life Support review and examination. After an excellent review of heart rhythms, various resuscitation drugs, much studying and fretting and sweating bullets while taking the written exam, I was taken into a small room by a seasoned and tough-as-nails intensive care unit nurse. There, on the table, lay Resusianne. After many years of saving her life, I just call her Anne for short. I don’t really care for her much but only because she makes me so nervous. You see, she is always trying to die on me.
Resusianne lives yet again.
My nurse examiner starts with the scenario that I’m in Nordstrom’s and come across a woman who is laying, unmoving on the floor. My first thought is sticker shock at the price of this bikini but I keep that to myself. I automatically go though the drill that has been beat into me over three decades.
“Anne! Anne! Are you okay?” Of course she’s not okay. Resusianne is never okay but it seems polite to ask. “I need help! Someone call 911 and someone bring an AED.” And then I start CPR. Now the fun starts when the AED arrives. I have to fumble for the on switch, rip open Anne’s shirt (fun!) and put on the paddles and then start CPR again until the AED tells me to stop. And then it seems like an hour before the AED decides to shock Anne. As soon as the shock is completed, I start in on CPR again until the nurse has mercy on me and tells me I can stop. Good CPR is really, really physical, especially for a petite little gal like me. By this time, I am a nervous wreck. I take Anne’s problems way too personally.
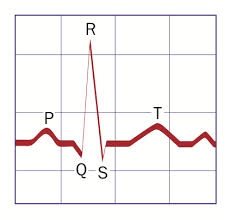
Normal Sinus Rhythm is a beautiful thing.
Next, my examiner gives me this scenario: I’m in the operating room with a patient and her EKG shows a heart rate that suddenly goes from 68 to 135 and her blood pressure starts to drop. This is the arrhythmia part of the test. You know that nice normal EKG pattern we always see with a spike between two humps? That is called normal sinus rhythm and that is what we love to see on an EKG but Anne is such a drama queen. She’s never in that rhythm for long. There are a dozen or so aberrant rhythms that range from kind of ugly to downright terrifying. Her current rhythm is somewhere in the middle and responds to a nice dose of Adenosine. She converts to normal sinus rhythm. Woo Hoo! But there she goes again. Fie on her. I give her a second and larger dose of Adenosine which really works this time. After Anne is conscious, I tell her that I will never, ever operate on her again and that she needs to find another plastic surgeon with larger cajones than mine.
And then my examiner raises the bar. This time Anne has just walked into my office to get her tummy tuck stitches out and she goes to ground right in the middle of my really nice waiting room! How rude. I go through all the steps of CPR and get EKG monitoring set up which shows normal sinus rhythm but Anne has no, nada, zero, zilch pulse. So now while I’m doing CPR and getting an IV started and pushing epinephrine I have to figure out why it is that Anne’s heart has electrical activity but is not pumping blood. There are about 12 reasons this can happen and I start with the most common in this scenario which is a pulmonary embolus (a blood clot to the lung). Now, after some IV fluid and epinephrine, Anne has a little bit of a blood pressure and I am ready to inset a breathing tube and get her over to Swedish Hospital for a diagnostic CAT scan and treatment and I’m about to have a cardiac arrest myself with my nurse examiner tells me that my exam is over and I passed! WOO HOO! I’m good for two more years and now I get to go change my scrubs which are soaked with sweat. I really, really hope I never have to use these skills. But I’m glad to keep up to date …..just in case. I say goodbye to the examiner but not to Anne. I may have a different examiner in two years but I know Anne will be back. She always is.
Thanks for reading and if you don’t know CPR, get thee to a class. The life you save my be of someone you love! Dr. Lisa Lynn Sowder
Seattle Plastic Surgeon and mother of a 14 year old daughter implores the naked cyclist at the Fremont Summer Solstice Fair to put a fig leaf on it.
I have been attending the Fremont Summer Solstice Fair for many years. I live just a few blocks away from Fremont, the self designated “Center of the Universe”. The fair is a fun and funky and freaky celebration of Seattle’s short but wonderful summer and just about anything goes. But this year, either I’m getting old and cranky or maybe the anything goes has gone too far.
Saturday’s parade has for years included a posse of nude cyclists who seem to appear from nowhere, weave through the parade and crowds and then disappear. And we all cheer for their naughtiness. But this year, after the parade, many of the cyclists just hung out, really hung out with nary a loin cloth. I felt like I was in a urology clinic. My daughter was having a hard time knowing where to look because everywhere she looked, there was another one.
So dudes, next year make sure you look for me. I will be the middle aged lady handing out free fig leaves for those of you who forgot yours.
Seattle Plastic Surgeon discusses options for upper arms.
The thermometer in Seattle is finally hitting 70 degrees after the most wretched sping in recorded weather history and I’m getting a lot of questions about upper arm enhancement.
The First Lady’s arms are the result of good arm genes and a great personal trainer. Also, she has not yet entered the menopausal years (more about that in a future post). For those without Mrs. Obama’s genes or trainer, there are a few procedures that can be done to improve the upper arm. Which procedure is the most appropriate is dictated by several factors:
Skin tone
Thickness of the fat layer
Condition of the underlying muscles
Scar history
Patients with a thin layer of fat and poor skin tone are usually older and thin. The only procedure that will improve the upper arm is a brachioplasty. This procedure involves removing the excess skin of the upper and inner arm. This always leaves a scar from the axilla (arm pit) to the elbow. I strive to keep this scar on the surface that is hidden against the side when the arms are down. The question patients must ask them selves is: “Am I willing to trade these bat wings for a scar?” In patients who heal well and the scar is narrow and light, the answer is usually “yes” but I do have one brachioplasty patient who has a lovely arm shape and excellent scars who is still too self-conscious to go sleeveless. I may have hit a surgical home run with her but I don’t consider the case a complete success.
Patients with chubby upper arms and good skin tone are great candidates for the CAST procedure. This procedure involves circumferential treatment of the arm with very careful tumescense power- assisted liposuction. The fat removal is limited to the outer arm where the excess fat resides but the inner arm is also treated with undermining the skin with the blunt liposuction cannula off of suction to stimulate shrinkage and tightening of the skin. Patients wear a compression bolero to help the skin tighten postoperatively.
Patients who are “in between” are often candidates for a combination procedure where the incision and resultant scar can be confined to the axilla and the very, very upper inner arm where the sun hardly ever shines.
So if you want perfect Mrs. Obabma’s arms, sorry it’s not likely to happen. But is you want better arms, there is likely something I can do to get you to your personal best.
If, like me, you are a fan of the cable T.V. show “Justified” you recognize this man as Johnny Crowder. I find him very attractive despite his really severe acne scarring. Maybe it’s because he is the quintessential bad boy or maybe it’s because he has such a soft heart despite being a total sociopath. Anyway, he was killed last season by his even more bad ass cousin, Boyd Crowder so I won’t be able to enjoy his handsome mug anymore. But this post is not about my taste in men but about acne scars.
Acne is often thought of as just one of the many challenges of adolescence and in many cases it is. Mild cases can often be controlled with over-the-counter treatments and usually the acne subsides once the hormones have leveled off. But for some, acne can be a devastating disease. When the acne lesions are deep and cystic, they can destroy the normal fat layer under the skin and cause deep permanent scars as in David Meunier, the actor who plays Johnny. Acne scars have not kept Mr. Meunier from finding success but they may limit his roles somewhat. He may find himself cast more frequently as a bad guy.
So if you or someone you know has out of control acne, get thee to a dermatologist. Those pesky “zits” of today can turn into the life long scars of tomorrow. Oh, one more thing – treating acne scars is really difficult and only partially effective. It’s much better to prevent them in the first place.
Thanks for reading! And Johnny, I miss you! Dr. Lisa Lynn Sowder
How are those planet lining up for your day of surgery?
Today I saw a lovely lady who is a great candidate for tummy tuck and fat transfer to the breasts. She’s done with babies, her youngest is out of diapers and she is ready to reclaim a little bit of her babehood. She’s also got some help lined up and some time off work available and now all she needs to do is check with her astrologer to make sure planetary alignment is just right!
Back when I was a smarty pants young surgeon, I would have dissed this lady’s belief in astrology but now that I have been around the block a time or two, I recognize that many people believe in things that I don’t and vice versa. So if I need to tweek my schedule a little bit to get in alignment with her planets, I’ll do my best to do so.
Thanks for reading and by the way, I’m an Aries. That explains everything, huh? Dr. Lisa Lynn Sowder
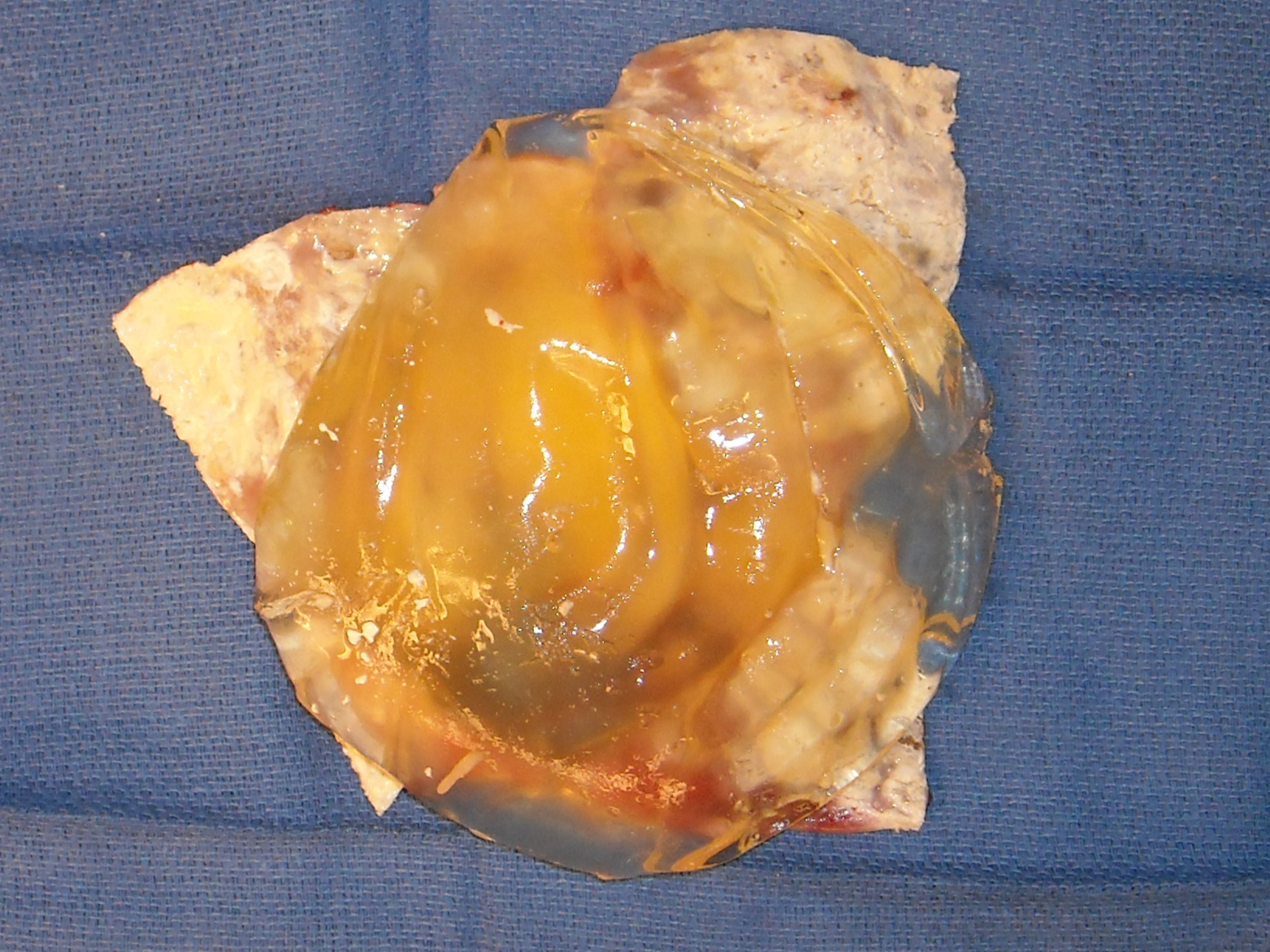
Calcified breast implant capsules can make a breast rock hard.
Calcified breast implant capsule surrounding an 32 year old ruptured silicone gel breast implant.
32 year old ruptured silicone gel breast implant after opening the calcified capsule.
I recently removed 32 year old breast implants from a lovely lady in her mid 60’s. She was embarrassed how the implants felt when she hugged someone. “It’s like having two rocks in my bra.” Here is the reason her breasts felt like rocks.
The photo on the top shows the implant surrounded by the implant capsule. The photo on the bottom shows the implant (which was ruptured) and the capsule after the capsule was opened. The yellow gooey stuff is the implant material. The white structure under the implant is the inside of the capsule. The white stuff is calcium. Yes, calcium – the same stuff that makes your bones nice and hard. The calcium deposits are hard and brittle and can make an encapsulated implant literally rock hard. Nasty capsules such as this are most common in old silicone gel implants but I have also seen cases like this in saline breast implants.
These photos also illustrate another important point with removal of ruptured breast implants. In this case, I was able to remove the ruptured implant and the capsule in one tidy piece and there was no spillage of the silicone into the breast. I love it when I can do this. It is not always possible but I always try. When it is not possible and I have to remove the ruptured implant before removing the entire capsule, there is often some spillage but I do my best to minimize it and clean up any spilled silicone prior to closing the breast.
And yet another important point should be obvious from this photo. Should the capsule be removed along with the implant? YES! It would be crazy to leave that nasty capsule behind. It would shrivel up into a hard mass, be palpable and possibly visible and would look really, really funky on mammogram. I always go after thick and nasty capsules. If removing the capsule puts a vital structure at risk, I may leave some of it behind but I try to get as much out as possible. Removal of the capsule is the hard part of the case but it is worth the effort and time to leave behind a nice, clean breast.
Oh, and one more point. This were really old implants. The implants available currently are much tougher and have thicker gel and are less likely to rupture. The problem illustrated with this case are less likely to occur with the new generation of implants.
Seattle Plastic Surgeon wishes everyone a Very Merry Christmas.
The Christmas season is always super busy in my practice. It seems crazy to have surgery around the holidays but it is the choice of many, many patients. They already have time off of work or school for recovery.
In my 23 years of practice, I have only taken time off around Christmas twice; once to take care of my newborn daughter and once to have surgery myself.
So Merry Christmas to everyone. I’ll be working every day except for Christmas, New Years Eve and New Years! It’s a good thing that I love my work!
Thanks for reading and stay tuned for some upcoming New Year’s Resolutions.
Okay, I have never seen his TV show but I do read his column in O Magazine every month and more often than not, I think to myself – really, how can you know that Dr. Oz????? You see he makes these big proclamations like: if you eat blueberries, you won’t get Alzheimer’s disease. And my scientific mind starts thinking about the kind of research it would take to prove that. Lets see – get 10,000 50 year olds and make half of them eat blueberries every day and then do brain biopsies on them when they are 65 to see if they have the plaques and tangles seen in Alzheimer’s disease. Ready to sign up for that one? That study has never been done and never will be done. Nor have or will a bajillion studies necessary to back up what Dr. Oz spews as medical fact.
Well, yesterday I had my sneaking suspicion confirmed that all of his spewing was mostly malarkey. Check out this article in the LA Times. Seems that only 11 % of what comes out of Dr. Oz’s mouth has any basis in reality and the rest, well, I guess he just makes it up as he goes. Okay, okay. He is an honest-to-God heart surgeon so I’m sure he knows a lot about hearts but geeze, all of this other stuff? Methinks someone just feeds him the lines and he spews them and gets away with it because he looks so hot in surgical scrubs.
Thanks for reading and my blog might not meet the highest standard of scientific inquiry, but it’s mostly true stuff most of the time! Dr. Lisa Lynn Sowder.










 @lisalynnsowder
@lisalynnsowder
