This is a question posted by a patient on RealSelf. She’s a lady in her 50’s with 11 year old anatomic Allergan Style 410 implants. She has typical menopausal symptoms and does not think her implants are causing her night sweats, mild brain fog or hot flashes. She’s heard about BIA-ALCL and wants to know if she should have her implants removed. The photos she submitted show an absolutely beautiful long term result and the rest of her looks pretty awesome too. She’s obviously either biologically privileged or she’s a gym rat or maybe both. She’s very lean. She doesn’t have enough fat for a meaningful fat transfer. Her breast volume is mostly implant. She loves her implants but she is scared. What should she do?
So let’s be rational about the advice we give her based on what we know about BIA-ALCL. First of all, she cares about her appearance. Will she look good after explant? IMHO, no. She will be very, very small breasted. If she’s okay with that, fine. But I don’t think she will be okay with it.
What are the odds that she will get BIA-ALCL? The latest numbers coming out of Dr. Mark Clemen’s work at MD Anderson estimate the chance of her developing BIA-ALCL is about 1 in 3000. What about the chances of her DYING from BIA-ALCL? Well, with increased awareness, early diagnosis and proper treatment, those chances are approaching ZERO. I cannot rationally recommend she part ways with her awesome and great looking implants for those odds.
Now let’s look at breast cancer. What are the odds? Well, about 1 in 8 or 9 women will be diagnosed with breast cancer. The cure rate for breast cancer is much lower that the 90% plus cure rate for early diagnosed and properly treated BIA-ALCL. Do we recommend bilateral prophylactic mastectomy for your average patient with average breast cancer odds? Of course we don’t. Women should be freaking out about the fact that they have breasts instead of the fact that they have textured breast implants! And this post is in no way dismissing the suffering and, yes, death of patients with delayed diagnosis and/or treatment of BIA-ALCL. These numbers mean nothing to someone who has died or lost a loved one BIA-ALCL. We now know so much more about the etiology, diagnosis, prevention and treatment of this really weird malignancy.
So this is what I would advise this lady if she were my best friend or sister: Her implants are getting up there in years. I would get them removed and replaced with smooth, round cohesive gel implants. With her anatomy she will look fine with round implants. It’s been demonstrated very well that anatomic implants offer almost zero benefit over round implants in patients with normal anatomy. If her surgeon finds seroma fluid or capsule nodules, he/she should do a capsulectomy and send the fluid and capsules for examination. If the capsule is smooth and thin and unremarkable, he/she can just adjust the implant pocket if necessary to accommodate the new implant and leave the existing capsule in place.
And then she needs yearly exams and regular mammograms based on her breast cancer risk.
Thanks for reading and I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
I’ve now been doing fat transfer to the breast for over seven years. I remain enthusiastic about this procedure in patients with favorable anatomy and realistic expectations. One FAQ relates to changes in the breast with weight changes. So here is what I have observed so far in my practice:
Yo-yo is a no-no for fat transfer!
If patients lose weight, the transferred fat shrinks and the patient loses volume in her her breasts. This also goes for patients who lose fat but maintain their weight. I have seen this in a couple of patients who did not have a major weight loss but who really leaned out with vigorous exercise. They both became Crossfitters and both lost a lot of the volume they gained after fat transfer. One went on to have implants. The other did not. I am thinking about adding “do not join Crossfit” to my post-op instructions!
Conversely, if a patient gains weight, the fat that was transferred to the breasts will expand and the breasts will get larger. I have seen this in a couple of cases. One case was a middle aged flight attendant who gained about 7 lbs on a cruise (this is why I do not go on cruises!) and became alarmed at how large her breasts became. I assured her that her breasts would go back to their pre-cruise size when she lost that extra weight and indeed they did. In another case, a patient gained just a few pounds and rather than going to her saddle bags as it usually did prior to fat transfer, she was delighted to see that it mostly went to her chest!
So whenever we are moving fat around, it’s best to have surgery when you are at a healthy and sustainable weight. I do not recommend fat transfer in patients who yo-yo. Significant weight fluctuations make for fluctuating results.
Thanks for reading and did you notice I did not say “ideal” weight? Sustainable and healthy weight is more important and more obtainable than ideal for most of us who are over 25 years old!
Dr. Lisa Lynn Sowder
I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity.
My last blog discussed the difficult and frustrating problem of capsular contracture of breast implants. As with just about every problem known to mankind, prevention is the best approach. But despite doing everything correctly pre-operatively, intra-operatively and post-operatively, a small number of patients will experience capsular contracture.
First a little history: Way back when the Earth was cooling and breast implants were the newest and coolest thing, surgeons would treat capsular contracture by “popping” the breast, the so-called manual or closed capsulotomy. Here is how it worked. The surgeon would take his great big strong paws and basically mash the poor breast until there was a pop and the breast went soft as the scar capsule ruptured and released its pressure on the implant. As you can imagine, there was a lot of moaning and screaming in the exam room during this process. It wasn’t long before surgeons realized that: 1. the capsular contracture always came back, 2. this can rupture a breast implant, 3. this can cause acute bleeding and 4. women don’t like being manhandled this way. I was just starting my training in plastic surgery just as manual capsulotomy was falling out of favor. I’m happy to say that I have never done this crude procedure and it is likely that I would not have succeeded had I tried. I have teeny tiny and not-so-strong hands. I would have likely ruptured one of my tendons before rupturing a capsule or implant.
Okay, that was then and this is now. For early capsular contracture, it’s worth trying medication. A dozen or so years ago it was observed that implant patients on a certain kind of asthma medication has a very low rate of capsular contracture. These medications are leukotriene receptor antagonists and they work for asthma by reducing inflammation. And inflammation is thought to be the final common pathway to capsular contracture. The two medications used are zafirlukast and mohnelukast. Accolate and Singular are the brand names respectively. I have had several patients resolve an early capsular contracture with these medications. I have also had a few patients who did not respond to these medications
These implants were 41 years old and had a grade 4 capsular contracture. I removed them and the capsule and inserted new implants. She is shown 18 months after surgery.
Once a capsule is well established, surgical intervention is the only way to resolve it. Complete capsulectomy removes the scar tissue and then the question is how to prevent a recurrent capsule. And does it make sense to just pop in another implant right away? This is just such a difficult question because none of us has a crystal ball to tell the future. Sometimes capsulectomy and a new implant works great but sometimes another capsular contracture starts forming despite doing everything right. Sometimes we create a new pocket and make a pocket under the muscle if the over the muscle implant had a capsular contracture and vice versa. Adding Accolate or Singular makes some sense. Sometimes adding a piece of acellular dermal matrix like Strattice (which should be spelled $$$$trattice) will decrease the chance of another capsule. And whenever there are several different approaches to a difficult problem, you can be sure that none of them works every time.
The only surgery I know of that will for sure prevent another capsular contracture is implant removal and total capsulectomy without implant replacement. This definitive treatment is readily accepted by many of my older patients who are sick and tired of their nasty, rock hard and uncomfortable implants. They look forward to being implant free. For younger patients, however, this can be a very, very difficult thing to accept, especially if they were really, really flat to begin with. I have at least one patient that comes to mind who had several capsular contracture related surgeries by me and finally we just threw in the towel and removed her implants along with her capsules. Her breasts returned pretty much to their preoperative size and shape but let me tell you, her wallet was never the same. A problem with capsular contracture can be very, very expensive and result in a lot of down time – off work, off exercise, off fun. This particular patient went on to have some fat transfer several years later and did well. She and I are both glad to have her implant saga behind us.
Just writing this post makes me feel like I never want to do another breast augmentation! And then I think of the patient I saw in clinic this morning. She was very, very flat chested and was too lean to consider fat transfer. I inserted 250 cc low profile cohesive gel implants last week and this morning I could not wipe the smile off her face. I think as long as there is Victoria’s Secret, there will be a demand for breast augmentation. I am just grateful that implant technology keeps improving as does our surgical technique. Hopefully sometime in the near future capsular contracture will be of historical interest only.
Thanks for reading and I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
Anyone who knows my practice well knows that I am not a big fan of breast implants. I much prefer fat transfer and/or breast lift to get a breast looking nicer. But sometimes only a breast implant will get the patient the size and shape of breasts they desire. Implants have many issues including malposition (too high, too low, too whatever), size problems (too big or too small), leaking or rupture problems. Those issues can usually be address with revision surgery. There is one issue that has tortured plastic surgeons and their patients from day one of breast implants decades ago. That problem is capsular contracture.
All implants develop a capsule. Actually it is the body that develops the capsule. This is normal reaction to a foreign body and, yes, breast implants are a foreign body, a large foreign body. A capsule only becomes a problem when it become thick and/or tight. As the capsule thickens or tightens, it puts pressure on the breast implant and turns any shape or profile of implant into a sphere because a sphere is the shape that supports the largest volume in the smallest surface area, or something like that. Geometry was a while ago for me! Thus most badly encapsulated implant all look sort of the same – like a ball. And they all feel hard, sometime really hard and often they are very uncomfortable. Capsules can even become calcified in which case the implanted breasts are literally rock hard.
Capsular contracture: Looks bad, feels bad.
So what causes capsular contracture? Good question and I hope the smart researcher who breaks the code wins the Nobel Prize in medicine some day. A lot of progress has been made, especially in the past 10 years or so and it sure seems like inflammation is the common pathway to capsular contracture. The most common causes of inflammation around the implant and resultant capsular contracture are 1. bleeding in the implant pocket, 2. subclinical infection and biofilm in the implant pocket, 3. leakage or rupture of silicone gel implants. Let’s look at these a little closer.
Bleeding in the implant pocket has been known to result in capsular contracture for decades. Plastic surgeons take a lot of care to really “dry up” the implant pocket prior to inserting an implant. This is usually done with an electrocautery device call a Bovie. This little gizmo allows the surgeon to zap little oozing vessels and help prevent any significant blood from accumulating around the implant. Also, in the rare incidence of post operative bleeding around an implant, surgeons are very quick to take a patient back to the OR to “wash out” the pocket, find and treat the bleeding and reinsert the breast implant. Sometimes a very minor bleeds can avoid a trip back to the or but in cases like these, the surgeon is on high alert for capsular contracture.
Subclinical infection and biofilm have been on our radar screen for 10 years or so. Biofilm (which deserves it’s own blog post) is a slimy substance that is produced by certain types of bacteria. It serves as a protective hiding place for bacteria and is resistant to antibiotics. The most common example of biofilm is dental plaque. Yuck. Anyway, once the biofilm issue became well known, much more attention was paid to reducing the exposure of implants to bacteria. We are now compulsive about washing out the implant pocket with antibiotic solution, using a no touch technique with a Keller funnel when inserting the implant, changing gloves prior to touching an implant and such. Remember the billionaire Howard Hughes and his OCD about germs? Well, we really go totally Howard Hughes with implant surgery! Also, the location of incision has been shown to have an effect on the rate of capsular contracture. Incisions around the nipple, through the arm pit or belly button have the highest rates of capsular contracture. Incisions under the breast (the inframammary fold) have the lowest rate. This is very likely due to a lower level of bacteria in the area of the inframammary fold as opposed to the other areas. I use the inframammary fold incision almost exclusively for this reason and also because it allows me to see the pocket really well.
Leakage or rupture of gel implants results the in silicone gel coming into contact with the capsule and this often seems to cause inflammation and hardening or tightening of the implant capsule. When I am going after a particularly nasty capsule, I expect to see an leaking or ruptured implant and I am usually not disappointed. The advances made in implant construction – thicker implant shells and more cohesive gel – will hopefully decrease this cause of capsular contracture.
So that is Capsular Contracture 101. Next up will be a blog about what can be done for capsular contracture. Stay tuned and thanks for reading. And I would be honored if you followed me Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
This weekend I had the opportunity to participate in a suture lab at Whitman College, a small liberal arts school in Walla Walla, Washington. This lab is designed for Whitman students who are interested in medical careers. The lab consisted of about 30 students and 7 doctors. The participating docs included one general surgeon, one plastic surgeon (moi), two OB-Gyns, two ER docs and one family practice doc.
Now you may be asking what the big deal is in tying a knot and that is a great question. Proper knots are important in surgery because an improper knot can come untied and the thing the suture was holding together will fall apart. Not good. Other activities that require proper knots that come to mind are rock climbing and boating. Knots need to hold. Also in surgery, it’s important to tie a knot that holds with the least amount of suture material. Excess suture material can be irritating to living tissue and can also harbor bacteria so you always want to use the knot that is just enough to do the job.
The first part of the lab involved showing the students how to tie two-handed knots and one-handed knots with a length of nylon cord. I immediately discovered how hard it was to teach a skill that I do without even thinking about it! I don’t need my brain because knot tying for me is now in my “muscle memory”, not in my head. It’s the same for many physical skills that involve repetition such as dancing, sports or playing a musical instrument. And I found that the more I tried to explain it, the harder it was to do. Fortunately I finally discovered I just needed to shut up and show the students how to do it and they were able to copy my movements.
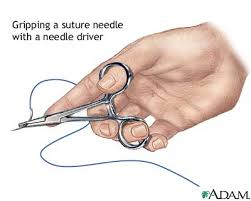
The next part of the lab was showing the students how to suture. For this we had a nice supply of pig’s feet. Pig skin is similar to human skin although thicker and tougher. Suture needles are different than a seamstress needle in that they are curved and require a instrument called a needle driver. The force required is very different than a simple push. It’s more of a stoke with a turn of the wrist. Again, I found explaining it very difficult because it all comes so automatically to me after all of these years. I was very impressed with the enthusiasm of the students and I think a number of them may very well make fine surgeons.
Another part of this visit included dining with the students in an informal lunch and dinner and answering their many, many questions about being a doctor. I found it bittersweet to compare my current position with theirs. I am nearing the end of my surgical career (I’m planning on 5 more years) and they are just at the beginning. They have so much uncertainty and so many challenges ahead. Most of that is now in my rear view mirror. I tried to give them some honest answers and not sugar coat the difficult pathway to becoming a doctor and in particular a surgeon. I really had a chance to reflect on all of those tough years of medical school and residency and the ongoing challenges of being in practice. I am envious of their youth but honestly would not want to trade places with any of them!
A real bonus for me was the information my 17 year-old daughter, who came with me, received from these bright college students. She is at the beginning of her college search and she got some great advice about choosing a college. And she got a nice tour of Whitman.
I am hoping I get invited back again to teach another batch pre-med students a few tricks of the trade. And who knows, one of those students may be my daughter!
Thanks for reading. Dr. Lisa Lynn Sowder
I would be honored if you followed my on Instagram @sowdermd and @breastimplantsanity.
If you look like this, you don’t need liposuction!
Taken from an article by Dr. Wayne Carman for online American Society of Plastic Surgeons from January 30, 2108
Liposuction is one of the most frequently performed cosmetic surgical procedures in the United States and around the world. This is somewhat surprising, considering how many misunderstandings about it persist. Listed below are the ten most common liposuction misconceptions we hear as plastic surgeons, and what the actual facts are.
Liposuction can help you lose weight
The reality is that most patients only lose about two to five pounds in total. The best candidates, in fact, are generally within 30 percent of a healthy weight range and have localized fat pockets they would like to reduce.
Liposuction can treat cellulite
Cellulite is not simply an irregular pocket of fat – it occurs when subcutaneous fat pushes connective tissue bands beneath the skin, causing those characteristic dimples and bumps. Because liposuction is only able to remove soft, fatty tissue (and does not directly affect the skin or other tissues), the fibrous connecting bands causing cellulite are not altered.
Liposuction is not for “older” people
Any patient who is in good health and has had a positive medical examination may safely receive liposuction. A lack of firmness and elasticity (both of which commonly decrease with age) may compromise the skin’s ability to re-drape over newly slimmed, reshaped contours. Poor skin quality is one of the main contraindications to liposuction.
Liposuction is dangerous
While every surgery carries an element of risk, liposuction techniques have become increasingly sophisticated. If performed by an experienced and board-certified plastic surgeon, and if the patient follows all appropriate postsurgical instructions, liposuction can be as safe and successful as any other surgical procedure.
Liposuction will fix lax skin
The appearance of a double chin or a heavy tummy may involve some degree of sagging skin with reduced elasticity, as well as excess fat. In such cases, your surgeon may recommend a skin tightening procedure instead of (or in conjunction with) liposuction, as liposuction alone may result in a deflated appearance.
Fat deposits removed will return after liposuction
Liposuction is “permanent,” in that once the fat cells are suctioned out, they will not grow back. However, there will still be some remaining fat cells that can grow in size and expand the area if one’s calorie intact is excessive. The best way to prevent this is to maintain a healthy diet and exercise regimen.
Liposuction is the “easy way out”
As mentioned earlier, liposuction is not a weight loss method, and maintaining ideal postsurgical results should include a general commitment to a healthy lifestyle. Liposuction (or any other body contouring method, for that matter) is targeted to streamline and contour localized areas – ideally, in someone who is within a healthy weight range.
You can get back to your routine right after liposuction
While relatively safe and frequently performed on an outpatient basis, every surgical procedure entails a recovery period, and liposuction is no exception. The most common after-effects include swelling, bruising, and soreness at and around the treatment areas. While the healing process varies from patient to patient, most should plan to take at least a week off work to rest and recover. It may be four to six weeks before a patient can resume strenuous activity or exercise.
Liposuction is only for women
Men frequently request liposuction – in fact, it was one of the top five most popular cosmetic surgeries American men received this past year, according to ASPS statistics. Common areas for treatment include the abdomen, love handles and chest.
Liposuction is always the answer to belly fat
Liposuction targets only subcutaneous fat – the kind that is located below the skin and above the muscle. An abdomen that protrudes due to fat under the muscle and around the internal organs (known as visceral or intra-abdominal fat) will not be improved with liposuction. Appropriate exercise and diet are the only effective methods to combat visceral fat.
Thanks for reading. Follow me on Instagram @sowdermd and @breastimplantsanity.
I see many, many women for implant removal after years of being unhappy with their breast implants. Many of these ladies consulted a plastic surgeon for sagging of the breasts and instead of ending up with a breast lift, ended up with breast implants. Often the explanation for this is that the patient did not want the “scars of a breast lift”.
So here’s the deal on breast lift scars. Yes, they are more extensive than the scars from an augmentation but,………………………..in the vast majority of patients, the scars fade to near no-big-deal status in about a year. Check out the example shown. The top photo is before a lift, the middle photo about 6 months post op and the bottom photo is one year post op. See the scar? Well you hardly can see the scars in the bottom photo. This is not an exceptional case. This is usually how it goes. Now there are some rare individuals who scar badly because of their particular biology but they are the exception.
So………….if you are saggy, you should get a lift. If you are really small you should get an augmentation with either an implant or fat transfer. As with everything, the correct diagnosis should lead to the correct treatment.
Thanks for reading and follow me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
I belong to a few physician only message boards and breast implant illness has been a hot topic in the past few months. It is interesting to see what other plastic surgeons think and especially what physicians in other specialties think about this controversial topic. These boards encourage free discussion without anyone being shut down, banished, blocked, or slammed on social media. This makes me grateful to be part of a group of professionals that value serious and candid discussion of complicated issues. Here I present a few thoughts I have curated from the past several months.
Dry eye and breast implants: Many, many ophthalmologists weighed in on this one. The consensus is that dry eye is very common in middle aged women. Women are 10 times more likely to develop dry eye. One doc said 80% of his female patients over 50 had dry eye. Conditions that contribute to dry eye include previous eyelid surgery (blepharoplasty), too much screen time, and some medications including SSRI antidepressants. Implants? No support for that theory from any of the ophthalmologists. My ophthalmologist, who recently did my cataract surgery, looked at me like I was nuts when I asked him about implants and dry eye. The eye docs also reminded us that silicone products are used extensively in ophthalmology: punctal plugs for dry eye, silicone stents for nasolacrimal duct reconstruction, silicone buckles used to treat retinal detachment, silicone oil used as a replacement for vitreous humor in the posterior chamber (eyeball), silicone intraocular lenses used after cataract extraction and finally silicone contact lenses. WOW. That’s a boat load of silicone.
When docs congregate is it wisdom of the crowd or groupthink?
Mold and biotoxins: General consensus from internal medicine and infectious disease is that patients ill with systemic fungal infections should be in the intensive care unit. None of the plastic surgeons, with one exception, had seen a case of mold growing in a saline implant. I added up the years of practice and it came to about 250 years. That is a lot of experience. One plastic surgeon who has written a book on BII seems to see mold and biotoxins wherever she looks. She puts her implant removal patients on extensive anti-fungal therapy post-operatively. She has extensive experience with mold and biotoxins but has not been published in any recognized peer reviewed medical journals. Her reason for not doing so has something to do with being targeted by Big Pharma. Hmmm.
Autoimmune issues: There were several rheumatologists weighing in on silicone triggered illness. Their opinions varied from no evidence whatsoever to there are some individuals who are genetically susceptible to autoimmune diseases (this is well known) and exposure to silicone may trigger the onset of disease in these individuals. It was noted that women are affected by autoimmune disease about 4 times more commonly than men. One infectious disease doctor thinks breast implants caused slceroderma (which is very, very serious connective tissue disorder and is usually fatal) in 6 of his patients. He recommended checking how wide an implant patient can open her mouth to diagnose early perioral and TMJ fibrosis and scleroderma. The rheumatologists thought that this doc was really out there. The plastic surgeon who has written a book on BII, who is not a rheumatologist, stated that rheumatoid arthritis is caused by an intracellular mycoplasma infection and she can cure rheumatoid arthritis and scleroderma with non-conventional therapy. None of the rheumatologists believed her. They all wondered why she had not published her results in a peer reviewed medical journal. Same answer. Big Pharma.
Breast Implant Associated Anaplastic Large Cell Lymphoma: It is rare. It is treatable if caught early. It is really creepy. It is associated with textured breast implants and/or tissue expanders. The plastic surgeon who wrote the BII book stated that BIA-ALCL was the most common cause of death in her implant patients prior to 2005. It was pointed out by several other doctors that BIA-ALCL was recognized as a disease around 2012.
Other stuff: Many of the internal medicine docs, ER docs, pain specialists, psychiatrists and OB-gyns weighed in on so called functional and somatic disorders including fibromyalgia, chronic fatigue syndrome, pelvic congestion, brain fog, anxiety, poor memory. depression, and malaise as primarily affecting women and pointed out that the vast majority of these women with these disorders do not have breast implants. This chatter of functional and somatic disorders made me think of the Freudian disorder of “hysteria” of yesteryear which was supposedly caused by the uterus wandering around looking for a baby. This sort of stuff gets my hackles up a bit, being a woman and all. One doctor wondered if there were any male to female transgender individuals with breast implant illness. Now that is a great question.
Future research: Everyone pretty much agreed that a large, multi-center, long term (10+ years) may help answer many questions about breast implants. Several plastic surgeons, myself included, pointed out that the dismal long term follow-up in previous studies was in part due to patient non-compliance with follow-up. I know this will make a lot of people angry but it is really true. Back when gel implants were only available through studies like the one I participated in, once patients had their coveted gel implant, they were gone, gone, gone. My follow-up for the McGahn study was about 80% which is really high because my staff and I pestered the participants mercilessly to come in for their appointments. Once doc suggested maybe a prison study using inmates with really long sentences. Maybe this could be Orange in the New Black meets Extreme Makeover?
Breast implants in general: Whoa, were there some strong opinions about this. Many, many non-plastic surgeons think any woman who gets implants is by definition is a mentally impaired bimbo. One doc divulged that his wife was going to get implants to treat her postpartum atrophy and boy did he get an earful! Many of the male doctors assumed that she was preparing to leave him once he had paid for her surgery! Such cynicism. But there was one family practitioner who has had the same set of implants for over 30 years (!) who said they absolutely changed her life. She went from a wallflower to a confident young woman. She even credits her implants for giving her the confidence to apply to medical school!
Plastic surgery and plastic surgeons in general: Some of the docs think that any sort of appearance altering surgery (except for obvious reconstructive procedures) was morally and intellectually bankrupt. This was an opinion shared by many anesthesiologists! Weird, huh? I wonder if my anesthesia group thinks they are slumming to work in my OR? I guess I should ask. Many of the male docs stated they didn’t need plastic surgery because their female partners found them totally smokin’ hot just the way they are. Hmmmm. Some of the docs think we plastic surgeons are a bunch of money grubbing fools. Oh well. I chalk that one up to jealousy. ; )
So there you have my carefully collected and curated review of some wild times on the doctor only message boards. You too can join a doctors only message board but first you have to finish medical school.
Thanks for reading and check out my Instagrams @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
K (Ryan Gosling) and the very evil Luv (Sylvia Hoeks) stroll among the newly finished small breasted replicants.
My husband and I went to Blade Runner 2049 this past weekend at Seattle’s wonderful Majestic Bay Theater. I am a big fan of the original Blade Runner thus the bar was very, very high for 2049. IMHO, Blade Runner 2049 was too frenetic, too convoluted and the only characters I really cared much about was Rick Deckard (the still handsome and wiley Harrison Ford) and his big ass shaggy mongrel doggie. I shed a tear when the doggie is shown peering out of a shattered building, wagging his tail just a bit, wondering where his human went. I’m tearing up now just remembering that scene.
One thing I found interesting throughout the movie was the relatively smallish breasts of all of the female characters. Hardly any cleavage at all – a real change for Hollywood. K’s (played by a deliciously disheveled Ryan Gosling) made-to-order AI concubine Joi (Anade Armas) and her human side kick, Mariette (Mackenzie Davis) with whom she mind and body melds, were both small chested. The LAPD’s Madame played by the ever wonderful Robin Wright was lean and mean and small chested. The still-under-construction and just “born” female replicants would all measure into an A or B cup bra. Even the gigantic virtual reality pleasure girl with the pastel hair was small breasted. The only bouncing breasts seen in the movie was in the cocktail lounge hologram dancing girls of the distant past. They contrasted nicely with Deckard and K beating the bejesus out of each other.
So maybe this return to a natural sized breast will be the next not-so-big thing for the ever scrutinized female figure?
Thanks for reading and if you haven’t seen the original Bland Runner, you are missing out on a great movie. Follow me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
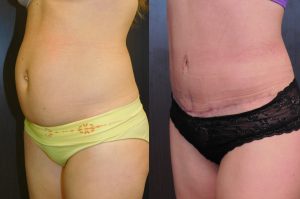
This patient had more muscle laxity that skin laxity. Here she is at 3 months with a very flat tummy. Her scar will fade with time.
I just love doing tummy tucks because this procedure allows me to tighten skin, fix muscle position, remove fat and improve a belly button in one operation. Usually this can be done with an incision that is admittedly quite long but is where the sun doesn’t usually shine. But sometimes, maybe 10% of cases, it is necessary to leave a scar in the lower mid-line. Sometimes a patient really needs a full tummy tuck to correct muscle separation but doesn’t have quite enough skin laxity of remove all of the skin between the pubis and the belly button and in those cases a “t-incision” is necessary. In most cases, I have a pretty good idea before surgery if I am going to need a t-incision but once in a while I cannot quite get that skin to stretch enough and have to leave a t-incision without prior warning to the patient. This occurred recently and I had a husband hopping mad at me for the extra scar. The alternative would have been to make the abdominal skin closure so tight that the patient would never be able to stand up straight again or position the really long horizontal scar quite high which would probably look worse than a nicely healed t-incision.
These intraoperative decisions are very, very difficult and sometimes, quite frankly, agonizing. I am hoping that this particular patient heals well and her vertical scar becomes a non-issue as is usually the case. And sometimes I just wish patients and their families could spend a day in my operating room clogs. It’s not so easy!
Thanks for reading and letting me get that one off my chest! Dr. Lisa Lynn Sowder
Follow me on Instagram @somdermd and @breastimplantsanity




 Many of these ladies consulted a plastic surgeon for sagging of the breasts and instead of ending up with a breast lift, ended up with breast implants. Often the explanation for this is that the patient did not want the “scars of a breast lift”.
Many of these ladies consulted a plastic surgeon for sagging of the breasts and instead of ending up with a breast lift, ended up with breast implants. Often the explanation for this is that the patient did not want the “scars of a breast lift”.


 @lisalynnsowder
@lisalynnsowder
