This is a question posted by a patient on RealSelf. She’s a lady in her 50’s with 11 year old anatomic Allergan Style 410 implants. She has typical menopausal symptoms and does not think her implants are causing her night sweats, mild brain fog or hot flashes. She’s heard about BIA-ALCL and wants to know if she should have her implants removed. The photos she submitted show an absolutely beautiful long term result and the rest of her looks pretty awesome too. She’s obviously either biologically privileged or she’s a gym rat or maybe both. She’s very lean. She doesn’t have enough fat for a meaningful fat transfer. Her breast volume is mostly implant. She loves her implants but she is scared. What should she do?
So let’s be rational about the advice we give her based on what we know about BIA-ALCL. First of all, she cares about her appearance. Will she look good after explant? IMHO, no. She will be very, very small breasted. If she’s okay with that, fine. But I don’t think she will be okay with it.
What are the odds that she will get BIA-ALCL? The latest numbers coming out of Dr. Mark Clemen’s work at MD Anderson estimate the chance of her developing BIA-ALCL is about 1 in 3000. What about the chances of her DYING from BIA-ALCL? Well, with increased awareness, early diagnosis and proper treatment, those chances are approaching ZERO. I cannot rationally recommend she part ways with her awesome and great looking implants for those odds.
Now let’s look at breast cancer. What are the odds? Well, about 1 in 8 or 9 women will be diagnosed with breast cancer. The cure rate for breast cancer is much lower that the 90% plus cure rate for early diagnosed and properly treated BIA-ALCL. Do we recommend bilateral prophylactic mastectomy for your average patient with average breast cancer odds? Of course we don’t. Women should be freaking out about the fact that they have breasts instead of the fact that they have textured breast implants! And this post is in no way dismissing the suffering and, yes, death of patients with delayed diagnosis and/or treatment of BIA-ALCL. These numbers mean nothing to someone who has died or lost a loved one BIA-ALCL. We now know so much more about the etiology, diagnosis, prevention and treatment of this really weird malignancy.
So this is what I would advise this lady if she were my best friend or sister: Her implants are getting up there in years. I would get them removed and replaced with smooth, round cohesive gel implants. With her anatomy she will look fine with round implants. It’s been demonstrated very well that anatomic implants offer almost zero benefit over round implants in patients with normal anatomy. If her surgeon finds seroma fluid or capsule nodules, he/she should do a capsulectomy and send the fluid and capsules for examination. If the capsule is smooth and thin and unremarkable, he/she can just adjust the implant pocket if necessary to accommodate the new implant and leave the existing capsule in place.
And then she needs yearly exams and regular mammograms based on her breast cancer risk.
Thanks for reading and I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
I get a lot of requests from breast implant illness patients to do an en bloc resection of their implants and the surrounding implant capsule. The term en bloc refers to a procedure that removes the structure in question in one piece or all together. This term is used most commonly in cancer surgery where a tumor is removed in its entirety without actually cutting into the tumor itself. Except in cases of BIA-ALCL, implant capsules are not cancer.
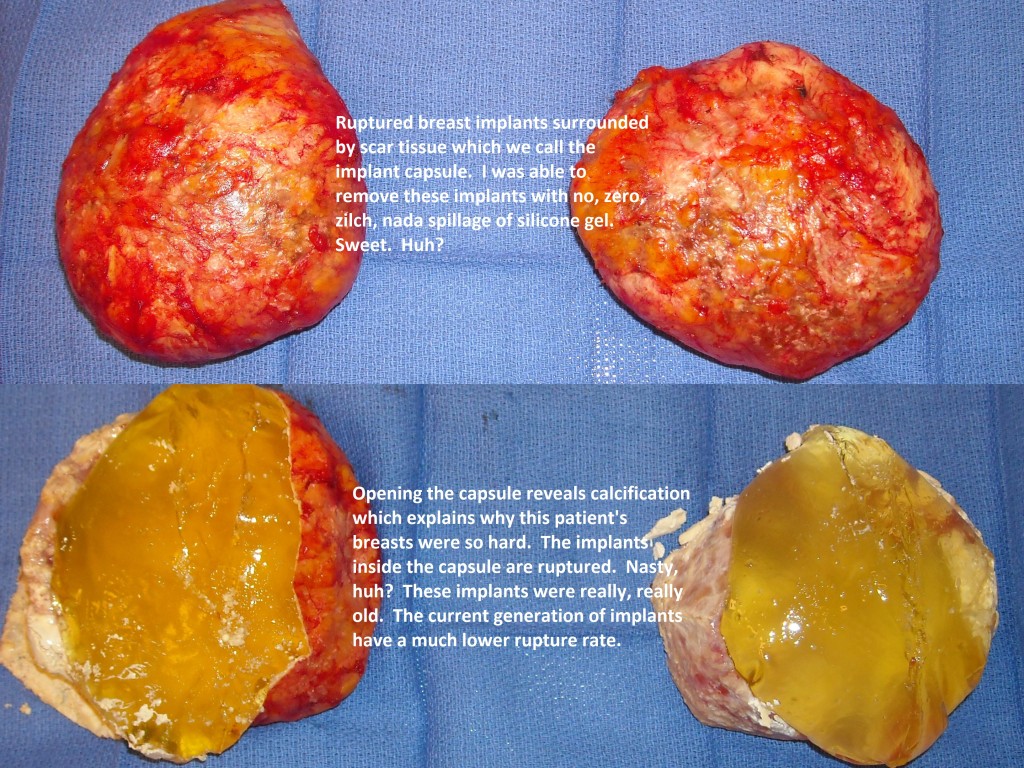
The photo below shows an en bloc resection of two ruptured breast implants and the surrounding capsule. In cases like this, doing an en bloc makes a lot of sense in that it prevents any spillage of silicone and makes for a much cleaner explant. Fortunately it is cases like this where an en bloc is usually doable. The thick, nasty and calcified capsule often just peels away from the adjacent breast tissue, muscle and chest wall without causing any collateral damage. Doing a clean and slick case like this is what surgeons live for and believe me, I wish every explant would go just like this!
But……….it is not always possible to do an en bloc resection. Sometimes the capsule is very, very thin and fragile (sort of like a wet Kleenex) and it is not possible remove it unbroken. Sometimes the capsule is very adherent to adjacent structures such as breast tissue, ribs and chest muscle. It is just not worth the damage to those normal structures to get an en bloc resection. Sometimes, with implants under the muscle, the patient is at risk for a collapsed lung when trying to peel a very adherent capsule from the rib cage. In cases like this, the capsule can be removed with curettage. And sometimes, with really large implants or those put in though the axilla (arm pit), the upper part of the capsule cannot be visualized with the implant in the way. And if I cannot see it, I will not cut it. In those cases, I remove the implant and then am able to safely remove the capsule. I am very careful about minimizing or, in most cases, eliminating spillage of any leaking gel.
I am aware that the breast implant illness community is obsessed with en bloc capsulectomy. I’m not sure why because for clean, intact implants, there is no compelling reason to do an en bloc, except maybe to show off and promote oneself, and yes, I am guilty of that! Many patients are lead to believe that there is some sort of evil humor or miasma that exists in the space between the intact and clean implant and capsule. The space (which is actually what we call a potential space because it contains nothing) contains nothing!
It is really easy to pontificate for a potentially dangerous procedure when one has zero responsibility for any downside. Who is responsible for harm to the patient – the surgeon holding the sharp instruments or the social media pundit?
And I am also aware that there are surgeons out there who guarantee an en bloc, every implant, every time. I honesty don’t know how they can. I also provide a guarantee… I’ll do my best.
Thanks for reading! Dr. Lisa Lynn Sowder
I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity.
This Friday one of my favorite drives on the planet will cease to exist. I know it’s silly to be attached to stretch of asphalt and concrete but I’m going to really, really miss the Alaskan Way Viaduct. For those of you who do not live in the Seattle area, the Viaduct is a big ugly, noisy and dirty double decker monster of a highway that is a blight on Seattle’s waterfront. But when I’m shifting my Minicooper into 5th gear on this monster, I feel like I’m flying through a magical landscape with a bursting young city on one side and a busy and beautiful waterfront on the other. On a clear day I feel like I could roll down the window and reach out to touch the Olympic Mountains to the west. It has the best damn view in Seattle and this view is available to anyone in a car or bus.
But alas, all good things must end, at least that’s the party line. This Friday night, barriers will go up, connections will be made to the deep bore tunnel that took many years to drill, and in a month, the big machines will come in to tear the Viaduct down. Over the next few years, Seattle’s waterfront will explode with new developments and I’m sure it will be awesome but I’m going to miss that big ugly magical asphalt ride.
Tomorrow, after work, I’m going to take one last ride and say goodbye. I’m sure I won’t be the only one.
Thanks for reading and I’d be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
Over the years, I have done a bajillion implant revision cases. This comes with the territory of being in practice many years (27 years and counting as of this blog post!) and also with showing and voicing an interest in revisional surgery. Implant revision is a fact of life. Breast implants are not life time devices and in general what goes in must eventually come out. Here a primer on the vocabulary of breast implant revision. Your surgeon may throw around these terms. Make sure you understand what he/she is saying and ask for clarification if you need to. Here goes:
Capsule: The scar tissue that forms around the implant. This happens with ALL implants. It’s a normal response to a “foreign body”. Yes, breast implants (like all non-biologic implants) are a foreign body.
Capsular contracture: The presence of a tight and often thick and sometimes calcified capsule. This results in a “hard implant”. This is abnormal scarring.
Implant pocket: The space where the implant resides. In cases of submuscular implants, the pocket is between the pectoralis major and the rib cage. In cases of subglandular implants, the pocket is between the breast gland and the pectoralis major. Sometimes a change in the implant pocket is advised for implant revision.
Implant malposition: Implants that are too high, too low, too medial or too lateral. This is most often corrected by modifying the implant pocket.
Bottoming out: A condition that occurs when the implant settles too low and/or is too loose.
Inframammary fold (IMF): The crease under the breast that is densely attached to the chest wall. The IMF tends to go back to where it was before implants after implant removal.
Double bubble: A condition that occurs when the implant falls below the inframammary fold. This is often accompanied by a crease along the lower breast at the level of the native inframammary fold or the edge of the pectoralis muscle.
Waterfall deformity: A condition that occurs when the implant stays put but the breast sags as it ages and falls over the implant.
Synmastia a.k.a. unaboob: Implants that are too close together. This looks really weird and is very, very hard to fix.
The gap: The space over the sternum that separates the breast. Sometimes the patients anatomy will result in a wider gap than she desires. Trying to close the gap can result in really lateral nipples or the dreaded unaboob. See above.
Capsulotomy: Cutting open the layer of scar tissue either to loosen it up or to change the position of the implant. This can sometimes be done with a local anesthetic.
Capsulectomy: Cutting out the capsule. This always requires a general anesthetic. This can be very difficult.
Capsulorrhaphy: Putting stitches into the capsule to either tighten it up and/or to raise the implant. This usually requires a general anesthetic.
En bloc capsulectomy: Removing the implant capsule with the implant without opening the capsule. This is the preferred method for removing a ruptured silicone gel implant. This is not always technically possible.
Acellular dermal matrix (ADM) and surgical mesh: A sheet of collagen or other substance that controls position of the implant and may prevent recurrent capsular contracture. Alloderm and Strattice are two of the ADMs I have used. I have also used Seri surgical mesh. Think of these as an internal bra, a very, very expensive internal bra.
Perfect symmetry: Not possible but we try.
Touch-up: This term best used when referring to make-up application. I try to avoid this term when it comes to breast implants. It implies that it’s easy and it’s never easy.
Revision: This term best used when referring to repeat surgery on a breast with an implant.
So there you have it. Now you can translate what your surgeon has told you needs to be done. And again, if you don’t understand make him/her go over it again until you do understand. Tell them Dr. Sowder told you to do so. Thanks for reading and I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity.
Recently I received this email from a former breast implant illness patient. I am sharing it with her permission but she has asked me to protect her identity. I will call her Celeste because I love that name. I have made no changes except for correcting a few typos.
Celeste: I read your blog post on breast implant illness and it literally brought tears to my eyes. Tears of joy!!!! Back up three or four years ago when my life was in shambles – emotionally abusive husband, stressed out to the max at work, sex hormones had crashed, possible thyroid issue…..but yet my family physician said I was fine according to my lab tests. I wasn’t able to see what my ex husband and stress were doing to my body at the time and so I was bound and determined to find an answer. Then I found it – the BII group on Facebook. I had found my answer so I thought. Went through the surgery and wow none of my symptoms got better! It wasn’t until my divorce was final and I was able to relax and started taking a low dose thyroid medicine and got my estrogen back to a normal level that I started to feel normal again. Long story short, I miss my implants like crazy and want them back. I’m soooooo happy to see a plastic surgeon standing behind her beliefs! I totally think it wasn’t my implants at all and more stress and hormone related. I guess I’m going to be the first trial case to see what happens. lol. Thanks for the blog. I really enjoyed it.
Me: I am very glad you are feeling better after getting your life in order and getting good medical care. Sorry about your implants, though. Have you shared your experience with the Facebook group? I am just curious.
Celeste: Hahahah. To spare myself the verbal attacking that would come with it, I have not. All of my friends have implants – a good mixture of saline and silicone, and none of them have issues. I even have one older friend who has had her saline implants for 20+ years to the point one ruptured and still no issues. I don’t want to fight with 18,000+ desperate women who are looking for an answer to their issues when in reality it is probably what you said, the general human condition and life itself. My mom has a lot of allergies and it is possible that my body reacted to my silicone implants (second set), but it took several years for me to feel bad. So, doubtful in my opinion. I had my saline implants for six years with no issues. The issues of general fatigue were once again a result of stress and being on birth control most likely. When I got my silicone implants I went off birth control and my stress was at an all time high. Perfect storm imo. But we shall see what happens. I’m torn on what to get again. I loved how my silicone looked and felt, but still have a slight fear that maybe just maybe it was my body reacting to the silicone (doubtful)……
I’m sure that group has attacked you. It’s like the blind leading the blind and defintely a herd mentality. I can’t bash them too much because three years ago I was one of them – desperate for an answer……and I’m a research scientist, so no dummy either ….. I was just that desperate to feel better.
Me: Is there any advice you would give women who like their implants but think they have breast implant illness?
Celeste: Oh geez this is a hard one. There is so much misinformation out there that if it seems pretty far fetched, it probably is.
I lived with my symptoms for years and even had my best friend, who is also my family physician, tell me that I was super stressed and THAT was my problem. The funny thing I have learned about stress in our society is that it starts out small and slow and that becomes the new normal. Then a little more stress gets added on, then that is the new normal. The cycle continues to repeat itself until something or someone stops it. In my case I got my second set of implants (silicone), stopped birth control causing my hormones to crash because I was basically dependent on it, major stress in my marriage, and I was studying for my board exams. And I was the silly one sitting in my doctor’s office telling her that I wasn’t stressed, but yet I couldn’t sleep, felt tired and heavy all the time, my weight was increasing quickly, etc. I went on like this for six years! I’m a little stubborn, ha! Removing my implants helped momentarily because allI could do was sit around and relax. That should’ve been my huge red flag. But nope, I missed it, lol. It wasn’t until just recently that all the pieces started coming together. My hormones are finally at normal levels, my stress is down, my divorce was final two weeks ago. I am finally relaxing and it feels good! I’m still going to the gym and doing strenuous weight lifting and from time to time when I don’t get enough sleep because I’m enjoying life too much and burning the candle at both ends, guess what????? My symptoms start to come back!
For me I’m skeptical that the millions of women that have implants are walking around like zombies (basically what I felt like). I was barely functioning – getting out of bed was difficult, but I didn’t want to lose my job so every morning was a struggle and a pep talk to do it one more day. And what about all the celebrities that have butt implants, chin implants, cheek implants, pec implants (men) – all silicone. I suppose one could argue that those are different than breast implants in chemical consistency, but why aren’t they feeling awful???? I’m more of a believer of an inflammatory response to implants that are too big for the body and overtime the body starts to reject them. My last set were DD and way too big imo. I’m naturally an A, so that is a big difference. And what about all the women in the bikini industry – models and competitors??? They are fine. I’m not saying breast implants are 100% safe, but causing issues almost a decade later is something that I’m not too sure on. My implants came out looking brand new with a thin capsule and no other issues. It is interesting though, the doc that took mine out says he’s seen some stuff that he just can’t explain and the lab can’t identify what it is……so maybe there is truth to it????
With all that being said, I think my biggest piece of advise is know that the mind is very powerful and when you are desperate for an answer, almost anything can be made to fit the given scenario. I wasn’t able to take a step back and evaluate my life and see that the problems I was having were self inflicted. Stress, abuse, lack of sleep, etc. had nothing to do with my implants. After years of living like this, my body was burned out and literally quitting on me. What it needed was lots of TLC! I’m still happy I got my implants removed. That set was too big, but I wish I would’ve swapped them out for a smaller set like my first set of implants. At this point I do miss my implants enough that I’m willing to risk that I’m completely wrong about all this and get implants again……..
So there you have it. Another side of the breast implant illness conundrum.
Thanks for reading and I would be honored if you followed me on Instagram @breastimplantsanity and @sowdermd. Dr. Lisa Lynn Sowder
In a previous blog post bemoaning the difficulty of good follow-up in clinical research I sort of place most of the blame on patients who blow off the follow-up once they have their desired implants. This was my experience with the implant study I participated in many years ago. I had an 80% follow-up at 5 years (which was really, really high) mostly because I pestered patients relentlessly to come back for their follow-up exams. I have taken a bit of flack (especially from the breast implant illness activists) for my blame-the-patient stance but now there is a recent study out that supports my politically incorrect opinion. Check this out. It seems if you pay the patient big bucks to show up they do! This study has an astounding 94.9% and 96.7% follow-up compliance at 5 years. The study has another 5 years to go and my guess is that given the size of the monetary award, those numbers will also be very high.
“Maybe I will show up for my follow-up.”
Novel Approach for Maximizing Follow-Up in Cosmetic Surgery Clinical Trials: The Ideal Implant Core Trial Experience
Mueller, Melissa A. M.D.; Nichter, Larry S. M.D.; Hamas, Robert S. M.D.
Background: High follow-up rates are critical for robust research with minimal bias, and are particularly important for breast implant Core Studies seeking U.S. Food and Drug Administration approval. The Core Study for IDEAL IMPLANT, the most recently U.S. Food and Drug Administration–approved breast implant, used a novel incentive payment model to achieve higher follow-up rates than in previous breast implant trials.
Methods: At enrollment, $3500 was deposited into an independent, irrevocable trust for each of the 502 subjects and invested in a diversified portfolio. If a follow-up visit is missed, the subject is exited from the study and compensated for completed visits, but the remainder of her share of the funds stay in the trust. At the conclusion of the 10-year study, the trust will be divided among those subjects who completed all required follow-up visits. For primary and revision augmentation cohorts, the U.S. Food and Drug Administration published follow-up rates from Core Studies were compared for all currently available breast implants.
Results: Five-year follow-up rates for the IDEAL IMPLANT Core Study are higher for both primary augmentation and revision augmentation cohorts (94.9 percent and 96.7 percent, respectively) when compared to all other trials that have used U.S. Food and Drug Administration standardized follow-up reporting (MemoryShape, Allergan 410, and Sientra Core Studies).
Conclusions: This trial demonstrates the utility of a novel incentive strategy to maximize follow-up in cosmetic surgery patients. This strategy may benefit future cosmetic surgery trials and perhaps any prospective research trial by providing more complete data.
CLINICAL QUESTION/LEVEL OF EVIDENCE: Therapeutic, IV.
Hey, thanks for reading and I really thank Drs. Mueller, Nichter and Hamas for this awesome article. And my hat is really off to Dr. Robert Hamas who not only thought up the idea of the Ideal implant but actually brought it to market. And Ideal only sells its implants to surgeons certified by the American Board of Plastic Surgery. That means if your surgeon is using an Ideal implant, he/she is actually a real honest to goodness plastic surgeon, not just poseur.
And I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
Surgical techniques are constantly evolving and breast implant technique is no exception. In the past couple of years recommendations to minimize implant and implant pocket contamination have been developed. This is in response to overwhelming evidence that bacterial contamination is the main cause of capsular contracture and may also be the cause of breast implant associated anaplastic large cell lymphoma (BIA-ALCL). Both of these conditions have been linked to the presence of biofilm around the breast implants. Biofilm is the product of certain bacteria, Staph epidermidis in the case of capsular contracture and Ralstonia piketti in the case of BIA-ALCL. It is our hope that with the adoption of the Surgical 14-Point Plan for Breast Implant Placement the annoying and difficult problem of capsular contracture and very serious and potentially fatal problem of BIA-ALCL will drop in frequency. If you are planning on breast implant surgery, you should ask your surgeon if he/she uses the 14 point plan. They should!
Surgical 14-Point Plan for Breast Implant Placement, from Aesthetic Surgery Journal, 2018, Vol38(6) page 625
Thanks for reading and I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
Occasionally I have a request from a patient’s friend or family member to come into the OR to “watch the surgery.” Many times they tell me that they have seen it on T.V. or on YouTube and just think it will be cool to see it in person. The answer is always no and here is why. In the OR, what may look like a relaxed and even fun atmosphere is actually a very carefully planned and executed choreography with several participants front stage and more in the wings. There is me and the scrub tech at the table and sometimes one of the 6th year plastic surgery residents from the University of Washington. Then there is the anesthesiologist keeping the patient asleep and safe and then there is the circulating nurse who helps the anesthesiologist and also opens equipment and supplies as needed. There really isn’t any extra room for a spectator and that spectator really isn’t going to see much because the surgical field is surrounded on all sides by anesthesia, the Mayo stand with the instruments and people on both sides of the table. And we keep OR “traffic” to a minimum because of infectious issues. The more people in and out of the OR the greater chance of contaminating the surgical field. And a lay person has very little concept of the sterile field and probably has not even heard the term “sterile conscious.” Don’t take it personally but we surgery types think lay people are just walking talking fomites.
“Jesus Christ! I think you are doing that wrong!”
And then there is “going to ground” factor. Even the most hardened lay person or even a doctor or nurse may react very differently to the sight of blood when that blood is that of a close friend or a loved one. If that person goes to ground, then we have another patient to take care of!
I have to tell just one little story about a would be OR spectator from my residency days. I was rotating at Children’s Hospital in Salt Lake City and doing an infant hernia case with the Chief of Pediatric Surgery, the wonderful Dr. Dale Johnson. One could not imagine a more competent and kind and ethical surgeon than Dr. Johnson. He was and even after retirement is a deity in surgery circles. We scrubbed our hands and arms and went into the OR for gowning and gloving. He noticed an extra person in the OR with a clipboard. (Surgeon’s have a visceral distrust of people with clipboards). Dr. Johnson politely asked this lady who she was and why was she here. She told Dr. Johnson that she was a “patient advocate” there for the patient’s protection. Dr. Johnson politely asked her from whom she was protecting the patient and if she was going to let him know if he was doing something wrong. She became flustered and just left the OR and I have never seen or heard of such a “patient advocate” since then. It was very strange and makes me think if a patient or patient’s parent think they need an advocate in the OR other than their operating surgeon, maybe they should choose another surgeon.
So go ahead and ask to be an observer but just be prepared to hear “no” in the nicest possible way.
Thank you for reading and I would be honored if you followed me on Intragram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
My last blog discussed the difficult and frustrating problem of capsular contracture of breast implants. As with just about every problem known to mankind, prevention is the best approach. But despite doing everything correctly pre-operatively, intra-operatively and post-operatively, a small number of patients will experience capsular contracture.
First a little history: Way back when the Earth was cooling and breast implants were the newest and coolest thing, surgeons would treat capsular contracture by “popping” the breast, the so-called manual or closed capsulotomy. Here is how it worked. The surgeon would take his great big strong paws and basically mash the poor breast until there was a pop and the breast went soft as the scar capsule ruptured and released its pressure on the implant. As you can imagine, there was a lot of moaning and screaming in the exam room during this process. It wasn’t long before surgeons realized that: 1. the capsular contracture always came back, 2. this can rupture a breast implant, 3. this can cause acute bleeding and 4. women don’t like being manhandled this way. I was just starting my training in plastic surgery just as manual capsulotomy was falling out of favor. I’m happy to say that I have never done this crude procedure and it is likely that I would not have succeeded had I tried. I have teeny tiny and not-so-strong hands. I would have likely ruptured one of my tendons before rupturing a capsule or implant.
Okay, that was then and this is now. For early capsular contracture, it’s worth trying medication. A dozen or so years ago it was observed that implant patients on a certain kind of asthma medication has a very low rate of capsular contracture. These medications are leukotriene receptor antagonists and they work for asthma by reducing inflammation. And inflammation is thought to be the final common pathway to capsular contracture. The two medications used are zafirlukast and mohnelukast. Accolate and Singular are the brand names respectively. I have had several patients resolve an early capsular contracture with these medications. I have also had a few patients who did not respond to these medications
These implants were 41 years old and had a grade 4 capsular contracture. I removed them and the capsule and inserted new implants. She is shown 18 months after surgery.
Once a capsule is well established, surgical intervention is the only way to resolve it. Complete capsulectomy removes the scar tissue and then the question is how to prevent a recurrent capsule. And does it make sense to just pop in another implant right away? This is just such a difficult question because none of us has a crystal ball to tell the future. Sometimes capsulectomy and a new implant works great but sometimes another capsular contracture starts forming despite doing everything right. Sometimes we create a new pocket and make a pocket under the muscle if the over the muscle implant had a capsular contracture and vice versa. Adding Accolate or Singular makes some sense. Sometimes adding a piece of acellular dermal matrix like Strattice (which should be spelled $$$$trattice) will decrease the chance of another capsule. And whenever there are several different approaches to a difficult problem, you can be sure that none of them works every time.
The only surgery I know of that will for sure prevent another capsular contracture is implant removal and total capsulectomy without implant replacement. This definitive treatment is readily accepted by many of my older patients who are sick and tired of their nasty, rock hard and uncomfortable implants. They look forward to being implant free. For younger patients, however, this can be a very, very difficult thing to accept, especially if they were really, really flat to begin with. I have at least one patient that comes to mind who had several capsular contracture related surgeries by me and finally we just threw in the towel and removed her implants along with her capsules. Her breasts returned pretty much to their preoperative size and shape but let me tell you, her wallet was never the same. A problem with capsular contracture can be very, very expensive and result in a lot of down time – off work, off exercise, off fun. This particular patient went on to have some fat transfer several years later and did well. She and I are both glad to have her implant saga behind us.
Just writing this post makes me feel like I never want to do another breast augmentation! And then I think of the patient I saw in clinic this morning. She was very, very flat chested and was too lean to consider fat transfer. I inserted 250 cc low profile cohesive gel implants last week and this morning I could not wipe the smile off her face. I think as long as there is Victoria’s Secret, there will be a demand for breast augmentation. I am just grateful that implant technology keeps improving as does our surgical technique. Hopefully sometime in the near future capsular contracture will be of historical interest only.
Thanks for reading and I would be honored if you followed me on Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder
Anyone who knows my practice well knows that I am not a big fan of breast implants. I much prefer fat transfer and/or breast lift to get a breast looking nicer. But sometimes only a breast implant will get the patient the size and shape of breasts they desire. Implants have many issues including malposition (too high, too low, too whatever), size problems (too big or too small), leaking or rupture problems. Those issues can usually be address with revision surgery. There is one issue that has tortured plastic surgeons and their patients from day one of breast implants decades ago. That problem is capsular contracture.
All implants develop a capsule. Actually it is the body that develops the capsule. This is normal reaction to a foreign body and, yes, breast implants are a foreign body, a large foreign body. A capsule only becomes a problem when it become thick and/or tight. As the capsule thickens or tightens, it puts pressure on the breast implant and turns any shape or profile of implant into a sphere because a sphere is the shape that supports the largest volume in the smallest surface area, or something like that. Geometry was a while ago for me! Thus most badly encapsulated implant all look sort of the same – like a ball. And they all feel hard, sometime really hard and often they are very uncomfortable. Capsules can even become calcified in which case the implanted breasts are literally rock hard.
Capsular contracture: Looks bad, feels bad.
So what causes capsular contracture? Good question and I hope the smart researcher who breaks the code wins the Nobel Prize in medicine some day. A lot of progress has been made, especially in the past 10 years or so and it sure seems like inflammation is the common pathway to capsular contracture. The most common causes of inflammation around the implant and resultant capsular contracture are 1. bleeding in the implant pocket, 2. subclinical infection and biofilm in the implant pocket, 3. leakage or rupture of silicone gel implants. Let’s look at these a little closer.
Bleeding in the implant pocket has been known to result in capsular contracture for decades. Plastic surgeons take a lot of care to really “dry up” the implant pocket prior to inserting an implant. This is usually done with an electrocautery device call a Bovie. This little gizmo allows the surgeon to zap little oozing vessels and help prevent any significant blood from accumulating around the implant. Also, in the rare incidence of post operative bleeding around an implant, surgeons are very quick to take a patient back to the OR to “wash out” the pocket, find and treat the bleeding and reinsert the breast implant. Sometimes a very minor bleeds can avoid a trip back to the or but in cases like these, the surgeon is on high alert for capsular contracture.
Subclinical infection and biofilm have been on our radar screen for 10 years or so. Biofilm (which deserves it’s own blog post) is a slimy substance that is produced by certain types of bacteria. It serves as a protective hiding place for bacteria and is resistant to antibiotics. The most common example of biofilm is dental plaque. Yuck. Anyway, once the biofilm issue became well known, much more attention was paid to reducing the exposure of implants to bacteria. We are now compulsive about washing out the implant pocket with antibiotic solution, using a no touch technique with a Keller funnel when inserting the implant, changing gloves prior to touching an implant and such. Remember the billionaire Howard Hughes and his OCD about germs? Well, we really go totally Howard Hughes with implant surgery! Also, the location of incision has been shown to have an effect on the rate of capsular contracture. Incisions around the nipple, through the arm pit or belly button have the highest rates of capsular contracture. Incisions under the breast (the inframammary fold) have the lowest rate. This is very likely due to a lower level of bacteria in the area of the inframammary fold as opposed to the other areas. I use the inframammary fold incision almost exclusively for this reason and also because it allows me to see the pocket really well.
Leakage or rupture of gel implants results the in silicone gel coming into contact with the capsule and this often seems to cause inflammation and hardening or tightening of the implant capsule. When I am going after a particularly nasty capsule, I expect to see an leaking or ruptured implant and I am usually not disappointed. The advances made in implant construction – thicker implant shells and more cohesive gel – will hopefully decrease this cause of capsular contracture.
So that is Capsular Contracture 101. Next up will be a blog about what can be done for capsular contracture. Stay tuned and thanks for reading. And I would be honored if you followed me Instagram @sowdermd and @breastimplantsanity. Dr. Lisa Lynn Sowder

 Alaskan Way Viaduct. For those of you who do not live in the Seattle area, the Viaduct is a big ugly, noisy and dirty double decker monster of a highway that is a blight on Seattle’s waterfront. But when I’m shifting my Minicooper into 5th gear on this monster, I feel like I’m flying through a magical landscape with a bursting young city on one side and a busy and beautiful waterfront on the other. On a clear day I feel like I could roll down the window and reach out to touch the Olympic Mountains to the west. It has the best damn view in Seattle and this view is available to anyone in a car or bus.
Alaskan Way Viaduct. For those of you who do not live in the Seattle area, the Viaduct is a big ugly, noisy and dirty double decker monster of a highway that is a blight on Seattle’s waterfront. But when I’m shifting my Minicooper into 5th gear on this monster, I feel like I’m flying through a magical landscape with a bursting young city on one side and a busy and beautiful waterfront on the other. On a clear day I feel like I could roll down the window and reach out to touch the Olympic Mountains to the west. It has the best damn view in Seattle and this view is available to anyone in a car or bus.




 @lisalynnsowder
@lisalynnsowder
